>Corresponding Author : Houssein Darwish
>Article Type : Case Report
>Volume : 3 | Issue : 1
>Received Date : 12 Dec, 2022
>Accepted Date : 22 Dec, 2022
>Published Date : 03 Jan, 2023
>DOI : https://doi.org/10.54289/JCRMH2300102
>Citation : Darwish H, Kawtharani S, Baajour J, Rahme R and Moussallem C. (2023) Metastatic Carcinoma to the Brain with Mucinous Features in a Patient in Remission with History of Breast Lobular Carcinoma Triple Positive: A Case Report. J Case Rep Med Hist 3(1): doi https://doi.org/10.54289/JCRMH2300102
>Copyright : © 2023 Darwish H, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Case Report | Open Access | Full Text
1Assistant professor of Neurosurgery, Division of Neurosurgery, American University of Beirut Medical Center
2Neurosurgery resident, Division of Neurosurgery, American University of Beirut Medical Center
3Medical student, American University of Beirut School of medicine
*Corresponding author: Nikolaos Andreas Chrysanthakopoulos, Oncologist (MSc), Specialized in Clinical Oncology, Cytology and Histopathology, Dept of Pathological Anatomy, Medical School, University of Athens, Athens, Greece Resident in Maxillofacial and Oral Surgery, 401 General Military Hospital of Athens, Athens, Greece
Abstract
Introduction: Breast cancer remains to be the most frequently diagnosed cancer in woman accounting for more than 2 million cases per year where it can metastasize to several organs in the body with brain metastasis being one of the most dreaded sequelae of it. Whole-brain radiosurgery, with or without surgical resection, or stereotactic radiosurgery remains to be the predominant treatment modality whereby surgical resection is limited to cases having a sole lesion identified or when located in excisable cortical regions.
Case description: We presented the case of a 71-year old female patient with history of Lobular carcinoma in situ triple positive with brain metastatic carcinoma with mucinous features consistent with breast origin while being in remission after she underwent bilateral mastectomies 6 years prior to presentation with negative PET scan for any lesion other than that in the brain.
Conclusion: Finding of brain metastasis with pathological features discordant with primary pathology of breast cancer, in a patient who is in remission years after undergoing bilateral mastectomies raises the question of the histological differentiation between the metastatic lesion and the primary source at the cellular level, and reflects on the relationship with receptor expression be it PR, ER or HER2.
Introduction
Breast cancer remains to be the most frequently diagnosed cancer in woman accounting for more than 2 million cases per year [1]. Advanced breast cancer can metastasize to several organs in the body with brain metastasis being one of the most dreaded sequelae of it [2]. In fact, it is considered to be the second most common metastatic cancer to the brain [3]. Broadly speaking, the overall incidence of brain metastasis in those with advanced breast cancer is around 10-30% [2]. The prevalence of brain metastasis has also been on the rise mainly due to the fact that patients have been surviving longer due to the advancement in treatment options [3]. Factors increasing the likelihood of brain metastasis are mostly related to tumor characteristics and include higher grade lymph node involvement at time of diagnosis, negative hormone receptor status, HER2 overexpression and basal phenotype [3]. In terms of treatment, whole-brain radiosurgery, with or without surgical resection, or stereotactic radiosurgery remains to be the predominant treatment modality. Surgical resection is limited to cases whereby a sole lesion is identified similar to our case, or when located in excisable cortical regions [2]. Systemic treatment such as chemotherapy and targeted immunotherapy can also be used [4].
Case Presentation
We present the case of a 47-year-old female patient, right handed, known to have a history of left breast mass to which she underwent bilateral mastectomy 6 years prior to presentation with pathology showing Lobular carcinoma in situ, ER, PR, and HER2 positive, with 20% Ki67 to which she received chemotherapy and hormonal therapy with no recurrence on regular follow up. She presented for dizziness and headaches to which MRI brain was done and showed left parietal ill-defined solid enhancing cortical tumor measuring approximately 2.3x 2.2 x 3.3 centimeter with strong contrast enhancement with surrounding vasogenic edema that has increased in size since previous examination causing mass effect on the adjacent sulci, involving the left post central gyrus (Figure). There is also associated leptomeningeal enhancement along the left post central sulcus extending inferiorly to the left superior temporal gyrus. The differential diagnosis included lymphoma versus metastasis. PET scan was negative for any lesion other than that in the brain. Lumbar puncture was done to rule out lymphoma and turned out to be inconclusive. Patient had intact neurological examination with no signs of Gerstmann syndrome. Left parietal craniotomy for tumor biopsy/resection was done. An inverted U skin incision was done, intraoperative ultrasound was used to confirm the lesion location. Tans-gyral resection was done using bipolar and micro-scissors. Fresh frozen was taken and was read by pathologist as metastatic carcinoma. Decision was made to continue with tumor resection. A clear plane was identified between the lesion and the normal brain and gross total resection was achieved. Post op pathology showed metastatic carcinoma with mucinous features consistent with breast origin.
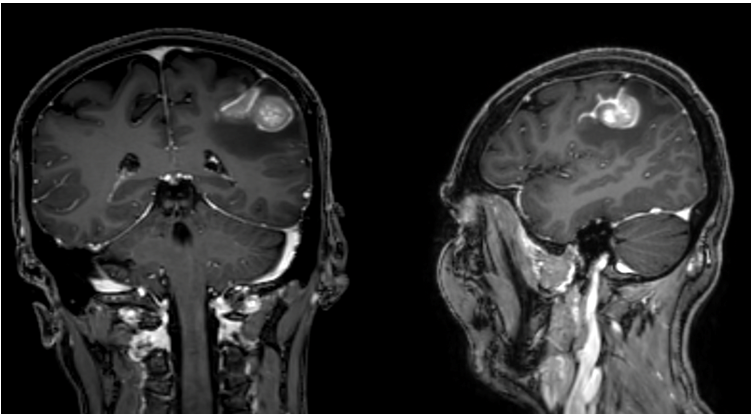
Figure 1
Discussion
Brain metastasis is most common in triple negative breast Ca (ER, PR and HER2 negative) whereby it occurs in around 46% of the cases, followed by HER+ breast cancer in 33% of cases, and only in 14% in the case of hormone positive disease [2]. Ductal carcinoma accounts for 80% of breast cancer cases followed by Lobular in 15% [5]. Ductal carcinoma is more commonly identified to metastasize to the brain where metastasis is more likely to occur in triple negative breast ca. In fact, pathology has identified invasive ductal carcinoma in 91% of cases with brain metastasis [4]. The two types of cancers, ductal and lobular, differ vastly in terms of histology, molecular as well as gene expression profiles and thus, have very different metastatic patterns [5]. Studies have delineated the presence of molecular discordance between the primary breast tumor and its metastasized lesion in up to 20% of the time [2]. Interestingly, Heterogeneity in the hormone receptor status and Ki67 LI were distinctly identified deprived of much morphological variability [6]. The predominant discordance found was the loss of hormone receptor expression and the gain of overexpression of HER2 [2]. Moreover, similar to other cells, breast cancer cells seem to acclimate to its surrounding microenvironment by developing neuronal characteristics such as expressing GABA receptors and transporters in act of homogenizing with the brain cells [2]. We presented the case of metastatic carcinoma with mucinous features consistent with breast origin in a patient in remission with history of Lobular carcinoma in situ triple positive. Our case stands out for several reasons. The patient showed metastatic lesion to the brain from a breast origin while the patient was in remission, with bilateral mastectomies done 6 years prior to presentation with negative PET scan for any lesion other than that in the brain. The patient’s pathology showed mucinous features which are not concordant with her primary breast pathology which was lobular in nature. The literature showed brain metastasis to be more present in triple negative patients and our patient had initial triple positive pathology with 20% Ki67.
Conclusion
Finding of brain metastasis with pathological features discordant with primary pathology of breast cancer, in a patient who is in remission years after undergoing bilateral mastectomies raises the question of the histological differentiation between the metastatic lesion and the primary source at the cellular level and reflects on the relationship with receptor expression be it PR, ER or HER2.
References
- Łukasiewicz S, et al. (2021) Breast Cancer-Epidemiology, Risk Factors, Classification, Prognostic Markers, and Current Treatment Strategies-An Updated Review. Cancers (Basel). 13(17). [PubMed.]
- Brosnan EM and Anders CK. (2018) Understanding patterns of brain metastasis in breast cancer and designing rational therapeutic strategies. Ann Transl Med. 6(9): 163. [PubMed.]
- Bailleux C, Eberst L and Bachelot T. (2021) Treatment strategies for breast cancer brain metastases. Br J Cancer. 124(1): 142-155. [PubMed.]
- Morgan AJ, Giannoudis A and Palmieri C. (2021) The genomic landscape of breast cancer brain metastases: a systematic review. Lancet Oncol. 22(1): e7-e17. [PubMed.]
- Korkola JE, et al. (2003) Differentiation of lobular versus ductal breast carcinomas by expression microarray analysis. Cancer Res. 63(21): 7167-7175. [PubMed.]
- Sava A, et al. (2021) Brain metastases originating in breast cancer: clinical-pathological analysis and immunohistochemical profile. Rom J Morphol Embryol. 62(2): 435-444. [PubMed.]