>Corresponding Author : Kerim Emre Yanar
>Article Type : Case Report Article
>Volume : 1 | Issue : 1
>Received Date : 4 August, 2021
>Accepted Date : 16 August, 2021
>Published Date : 20 August, 2021
>DOI : https://doi.org/10.54289/JCVR2100101
>Citation : Yanar KE, Ilgun M, Aydin O, Aktas MS (2021) Nasopharyngeal Polyp in a Cat: Clinical Assessment. J Clin Vet Res 1(1). doi http://doi.org/10.54289/JCVR2100101
>Copyright : © 2021 Yanar KE, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Case Report Article | Open Access | Full Text
1Ataturk University, Faculty of Veterinary Medicine, Department of Internal Medicine, Erzurum, Turkey
2Ataturk University, Graduate School of Health Sciences, Department of Veterinary Internal Medicine, Erzurum, Turkey
*Corresponding author: Kerim Emre Yanar, Ataturk University, Faculty of Veterinary Medicine, Department of Internal Medicine, Erzurum, Turkey
Abstract
The case report describes diagnosis and surgical treatment of nasopharyngeal polyp in a 3-months-old mixed breed female cat with sneezing, runny nose, lack of appetite and change of voice Serous tear discharge, mucopurulent nasal discharge and increased sensitivity in trachea were detected at clinical examination of the cat Following inspection of the oral cavity, it was observed that the soft palate was bulged and had a different appearance from the normal anatomical structure Significant alterations were not determined in the haematological, biochemical and radiographic examinations However, nasopharyngeal polyp was determined following the contrast-enhanced computed tomography examination After the polyp was removed by a simple invasive procedure, clinical findings of the cat started to improve as from the second day One month after the operation, the she was completely cured and became healthy In conclusion, nasopharyngeal polyp has to be considered for cats with lack of appetite, sneezing, runny nose and change of voice, and collaboration between oropharyngeal examination and transversal shots of the computed tomography would constitute a reliable approach for a precise diagnosis and preoperative planning for feline nasopharyngeal polyps.
Keywords: nasopharyngeal polyps; CT scans; benign
Abbreviations: FNP: Feline nasopharyngeal polyps, CT: computed tomography, MRI: magnetic resonance.
Introduction
Feline nasopharyngeal polyps (FNP) are benign, non- neoplastic, and stalked masses [1]. They originate from the eustachian tube or middle ear, and can spread into the nasopharynx, tympanic cavity, or both. This relatively rare disease was also called as inflammatory polyps, pharyngeal polyps, aural polyps, middle ear polyps, cats respiratory system polyps and oropharyngeal polyps [1, 2]. Although the etiology of FNP is not known for certain, it has been suggested that it may occur congenital or acquired, and the acquired cases may develop secondary due to nasopharynx- induced infections [3]. Although the disease is mostly encountered in young cats (mean age range from 136 months to 3 years old), it can also be come across in adult cats (mean age of 61 years old) [4]. There is no breed or gender predisposition. Similar polyps have been reported in horses and dogs [4, 5]. Clinical findings in cats with FNP include lack of appetite, weight loss, sneezing, runny nose, wheezing, dyspnea, dysphagia, ear discharge and nodding [1]. It may also have a history of a chronic upper respiratory tract infection. Although many cats have no history of nasal or ocular discharge, rhinitis or sinusitis may occur due to blockage of normal airflow [2]. Less commonly, cyanosis and syncope episodes can be seen, especially when large polyps block nasopharynx of the cats. Cats with FNP may show symptoms of otitis externa, otitis media or otitis interna [3, 6]. Diagnosis of FNP can be made by oropharyngeal examination, palpation of soft palate, skull graphs, endoscopy, computed tomography (CT), magnetic resonance (MRI) scans, nasopharyngeal biopsy or combination of these methods [7]. In addition, FNP can be diagnosed with clinical, rhinoscopic and immunohistochemical findings [8, 9]. Since the eustachian tube and tympanic cavity tissue are very similar to each other, histopathological determination of the origin of FNP is difficult. The treatment of the disease is accomplished by surgical intervention. In the treatment of FNP, simple operative attempts include withdrawal-avulsion, ventral bulla osteotomy along with ablation of the ear canal, and less frequently laser treatment [6]. The aim of this case report is to provide detailed information about the clinical findings, diagnosis and treatment of a cat with nasopharyngeal polyps.
Case History
A 3-month-old mixed breed female cat was referred to Ataturk University Veterinary Faculty Animal Hospital with complaints of sneezing, runny nose, lack of appetite and a change of voice. Clinical examination of the cat revealed that the body temperature was 387 ºC, the number of respiration was 18 per minute and the heart pulse was 185 per minute, as well as serous tear discharge, mucoprulent nasal discharge, increased sensitivity in trachea. Because of suspicion of upper respiratory tract infection, Amoxicillin clavulanic acid (Synulox enj®) was administered to the cat via subcutaneous injection with a dose of 1 ml/20 kg/day for 10 days After these injections, nasal discharge decreased and appetite increased slightly, but the clinical findings did not fully improve. After the antibiotic treatment was completed in our hospital, the cat was taken to another veterinary clinic, and steroids, antibiotics and diuretics were administered for 10 days. But the cat was not able to provide complete clinical improvement, and then she was brought back to Ataturk University Veterinary Faculty Animal Hospital The haematological panel (Abacus Junior Vet-5) (WBC, LYM, MON, NEU, BAS, EOS, LYM %, BAS %, MON %, NEU %, EOS %, RBC, HGB, HCT, MCV, MCHC, RDWc, PLT, MPV, PCT, PDWc, PDWs, RDWs) of the cat had a slight decrease in percentage of lymphocyte (1120 %) and a slight increase in percentage of neutrophil (8510 %), all other parameters were determined that they were within the range of reference values. The biochemistry panel (Randox) (urea, creatinine, ALT, AST, ALP, CK-MB, CK-NAC, GGT, LDH, amylase, total protein, triglycerides, cholesterol, glucose, uric acid, P, Mg, Ca, Cl) showed slightly increase in total protein (858 g/dl) and ALP levels (78 u/L), on the contrary of significant increases of glucose (407 mg/dl) and cholesterol (181 mg/dl) levels Radiological examination showed collapse in the trachea Streptococcus spp was isolated in bacteriological examination from sterile nasal swaps. As a result of the antibiogramme, it was determined that it was resistant to tetracyclines, susceptible to marbofloxacin, sulbactam ampicillin, amoxicillin clavulonic acid and ciprofloxacin.
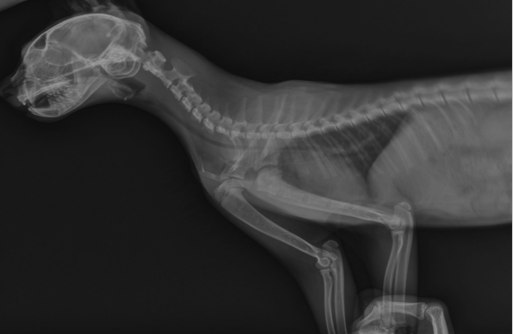
Figure 1: Tracheal collapse in radiological examination
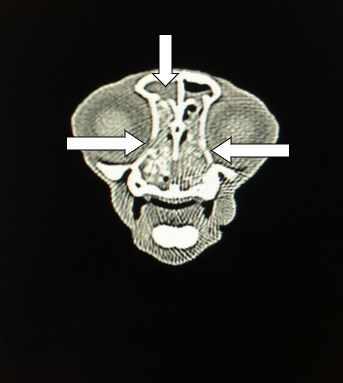
In contrast CT (Tomographic examination, shooting was done in transversal position in 1 mm sections Contrast substance, Ultravist® 300 mg/ml, 1 ml/kg dose 0 Per Second iv was applied) the presence of polyps in the ethmoturbinal region was detected (Figure 2a). The Transversal shot was also demonstrated partial destructions in the septa portion of the frontal sinus connected to the polyp, along with unilaterally nasal discharge in the frontal sinus (Figure 2b).

(a)
(b)
Figure 2 Transversal shot of CT with nasopharyngeal polyp (a) Partial destructions in the septa portion of the frontal sinus and unilaterally nasal discharge in the frontal sinus (b).
The oropharyngeal examination revealed that the soft palate was bulged and had a altered appearance than its anatomical structure. The polyp appeared when the soft palate was pushed towards the cranial, and the patient was diagnosed with FNP. It was decided to remove FNP using the minimally invasive interference method. For this purpose, intubation tube was applied after anaesthesia with propofol (slow intravenous dose of 3 mg/kg) was provided Polyp of the soft palate was removed with the aid of forceps (Figure 3).
After removing of the polyp, Marboflaxacin tablet (Marbocyl P®) for 5 days at 2 mg/kg/day dose orally and acetyl cysteine for 3 days at 70 mg/kg/day dose were administered intramuscular injection due to the intensity of discharge in frontal sinus. Prednisolone was not administered because the cat had been on steroids for 10 days at another clinic before being brought to our hospital. On the second day of the treatment, the patient's appetite, movement and interest for her surroundings started to increase and clinical findings improved considerably. There were no problems with the cat.
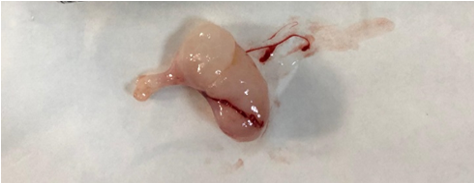
Figure 3: The Nasopharyngeal Polyp
FNP is the most common cause of non-neoplastic growths found in the nasopharyngeal region [5]. This condition is believed to be caused by persistent epithelial hypertrophy and submucosal proliferation following inflammation [4]. FNPs are the most common nasopharyngeal disease after lymphoma [3, 7]. In a retrospective study of nasopharyngeal diseases, 49% of 53 cats were diagnosed with lymphoma and 28% with polyps [10]. Although the etiology of FNP is not well-known, it may be secondary to chronic upper respiratory tract infections, chronic otitis media, nasopharyngeal infections or congenitally [1, 5, 7]. In a study on cats with FNP feline calicivirus was isolated from the nasopharynx of cats, while another study reported that neither calicivirus nor herpes viruses were responsible for the growth of NFPs by polymerase chain reaction from formalin-fixed polypoid tissue in cats with FNP [11]. Although the most common age of the disease in the literature is stated as from 136 months to 3 years, the fact that the cat in this case is at a very young age like 3 months suggests the possibility that the disease may have been occurred as congenital, and definitive opinion on etiology has not been reached.
The clinical findings of the disease are weight loss, lack of appetite, sneezing, cough, runny nose, nystagmus, ataxia, visible polyps, dyspnea, stridor, sound change, nodding, head bending, ear discharge, bad breath and dysphagia [8, 12, 13]. The clinical findings identified in the present case are similar to those reported. Although there is no specific finding in haematological parameters for cats with FNP, haematological changes occur for cats' upper respiratory tract infections [9]. In the present case study, no haematological changes were observed, despite of the diagnosis of dense sinus discharge in the CT image. It has been assessed that this result may be due to the antibiotics which was previously used. Similarly, although there is no specific biomarker in biochemical parameters for cats with FNP, it was determined that glucose and cholesterol levels were increased in this case study. It is assumed that the situation involved may be due to fullness of the cat which ate before taking the blood sample [14, 15].
FNP diagnosis for cats is performed by endoscopy, CT scan, head graphs, oral examination (with or without dental
mirrors), palpation of soft palate, nasopharynx biopsy or combination of these methods [7]. Radiography can be used to identify the soft tissue mass in the nasopharynx and to appraise the thickening of the wall and loss of normal air shade [16]. Standard lateral or standard oblique position is usually preferred for radiographic determination of FNP [17, 18]. However, mostly the radiographic examination helps for diagnosis for cats with otic polyps through showing loss of air contrast in the air canal and/or tympanic membrane, thickening of tympanic bone as well as presence of soft tissue mass in the pharynx or ear canal [5]. In some cats with FNP, radiographic examination may give normal graphics. In such cases, it is recommended that the diagnosis should be made with endoscopic examination or advanced imaging methods [5, 17, 18]. The graph taken in the present study demonstrated that collapse was shaped in both cervical and thoracic trachea (Figure 1), and this result could be attributed to tracheitis as reported by Sparkers [19]. In addition, it was suggested that the increase in sensitivity in trachea, which was determined in clinical findings in the present case, may have been resulted from tracheitis. Upper respiratory tract infections can lead to tracheitis [20]. In addition, the radiographic image taken in latero-lateral position did not show the presence of any mass in the nasopharynx in this case study, and the result was in accordance with literature findings [5]. It was noted that CT was more specific in early detection of small masses in the tympanic cavity and nasopharynx, and therefore, CT imaging was superior over conventional radiography [17]. In CT and FNP typically appear as a dense structure with a well-defined, rigid frame covering oval homogeneous space [5, 18]. More aggressive infections and neoplastic conditions often indicate both osteoproliferative and lytic lesions of the tympanic bulge. In contrast CT images, FNP exhibit a noticeable increase of the contrast material in these aggressive conditions. On the contrary to tomographic examination, the frontal sinus was filled with bilateral fluid and the presence of lytic lesions was determined in the etmoturbins. The runny nose, weakness and weight loss, and the frontal sinus filled with fluid that gives lower contrast are signs of an aggressive infection. In this case study, enhance of the contrast material in the etmoturbinal region was also observed by CT scans, and the finding was in harmony with results of the other researchers It was also suggested that the increase of the contrast material could be due to the mass [5, 18].
The most radical solution for the treatment of FNP is surgical intervention. Both minimally invasive and traditional surgical techniques are used to remove FNP. In minimally invasive attempts, towing/avulsion is the simplest method that can be applied without requiring special equipment. In this method, the polyp is held with a threaded grip forceps (curved clamp, Allis, or aligator forceps) and removed by rotating and pulling tightly until separated [6, 14]. In addition, FNP can be removed by endoscopy, laser ablation and open surgery, which are traditional surgical techniques. In the present case, FNP was successfully removed using minimally invasive interference method for the removal of FNP [8]. Use of antibiotics and prednisolone as postoperative care is recommended after removal of FNP. In this case, postoperative treatment was applied in accordance with the literature report. On the second day of the treatment, the patient's appetite, movement and interest for her surroundings started to increase and clinical findings improved significantly. One month after the operation, the animal owner informed us that there was no problem with the cat and that she was completely cured and healthy.
In conclusion, nasopharyngeal polyp has to be considered for cats with lack of appetite, sneezing, runny nose and change of voice, and collaboration between oropharyngeal examination and computed tomography would constitute a dependable approach for an accurate diagnosis and preoperative planning for feline nasopharyngeal polyps.
Conflict of interest: The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding: The authors received no financial support for the research, authorship, and/or publication of this article.
ORCID ID: K Emre YANAR https://orcidorg/0000-0001- 7302-7077.
References
- Galloway P, Kyles A, Henderson J. (1997) Nasal polyps in a cat. J Small Anim Pract. 38(2): 78-80. [PubMed.]
- Stanton M, Wheaton LG, Render JA, Blevins WE. (1985) Pharyngeal polyps in two feline siblings. J Am Vet Med Assoc. 186(12): 1311-1313. [PubMed.]
- Anderson DM, White RA, Robinson RK. (2000) Management of inflammatory polyps in 37 cats. Vet Rec. 147(24): 684- 687. [PubMed.]
- Veir JK, Lappin MR, Foley JE, Getzy DM. (2002) Feline inflammatory polyps: historical, clinical, and PCR findings for feline calici virus and feline herpes virus-1 in 28 cases. J Feline Med Surg 4(4): 195- 199. [PubMed.]
- Muilenburg RK, Fry TR. (2002) Feline nasopharyngeal polyps. Vet Clin North Am Small Anim Pract. 32(4): 839-849. [PubMed.]
- Rogers KS. (1988) Tumors of the ear canal. Vet Clin North Am Small Anim Pract 18(4): 859-868. [PubMed.]
- Davidson JR. (2014) Otopharyngeal/Otic Polyps in Cats Current Techniques in Small Animal Surgery. 2014: 232. [Ref.]
- Lamb CR. Sibbing K, Priestnall SL. (2016) Pathologic basis for rim enhancement observed in computed tomographic images of feline nasopharyngeal polyps. Vet Radiol Ultrasound 57(2): 130-136. [PubMed.]
- Moosavian HR, Esmaeilzadeh H, Vahabi R, Vafaei R, Esmailinejad MR. (2019) A nasopharyngeal inflammatory polyp in a cat: histopathology, immunohisto chemistry, and CT scan findings. Turk J Vet Anim Sci 43(1): p 167- 172. [Ref.]
- Allen HS, Broussard J, Noone K. (1999) Nasopharyngeal diseases in cats: a retrospective study of 53 cases. J Am Anim Hosp Assoc 35(6): 457-461. [Ref.]
- Parker NR, Binnington AG. (1987) Nasopharyngeal polyps in cats: three case reports and a review of the literature. J Am Animal Hosp Assoc. 21(4): 473-478. [Ref.] [PubMed.]
- Bradley RL. (1984) Selected oral, pharyngeal, and upper respiratory conditions in the cat Oral tumors, nasopharyngeal and middle ear polyps, and chronic rhinitis and sinusitis. Vet Clin North Am Small Anim Pract. 14(6): 1173- 1184. [PubMed.]
- Varshney H, Varshney J,Biswas S, Ghosh SK. (2016) Importance of CT scan of paranasal sinuses in the evaluation of the anatomical findings in patients suffering from sinonasal polyposis. Indian J Otolaryngol Head Neck Surg. 68(2): 167- 172. [Ref.]
- Greci V, Mortellaro CM (2016) Management of otic and nasopharyngeal, and nasal polyps in cats and dogs. Vet Clin North Am Small Anim Pract, 2016 46(4): p 643-661. [PubMed.]
- Bedford PG, Coulson A, Sharp NJ, Longstaffe JA. (1981) Nasopharyngeal polyps in the cat. Vet Rec 109(25-26): 551- 553. [PubMed.]
- Cox N, Brawner WR, Powers RD, Wright JC. (1992) Tumors of the nose and paranasal sinuses in cats: 32 cases with comparison to a national database (1977 through 1987). J American Animal Hosp Assoc. 27(3):339-347. [Ref.]
- Landsborough L. (1994) Nasopharyngeal polyp in a five-month-old Abyssinian kitten Can Vet J. 35(6): 383-384. [PubMed.]
- Tanaka T, Akiyoshi H, Mie K, Nishida H. (2018) MRI findings, including diffusion- weighted imaging and apparent diffusion coefficient value, in two cats with nasopharyngeal polyps and one cat with lymphoma. JFMS Open Rep. 4(2): 2055116918812254. [PubMed.]
- Reed N, Gunn-Moore D. (2012) Nasopharyngeal disease in cats: 1 Diagnostic investigation. J Feline Med Surg. 14(5): 306-315. [PubMed.]
- Bischoff MG, SK Kneller. (2004) Diagnostic imaging of the canine and feline ear Vet Clin North Am Small Anim Pract. 34(2): 437-458. [PubMed.]