>Corresponding Author : Oluseun Olufade
>Article Type : Research Article
>Volume : 1 | Issue : 1
>Received Date : 29 September, 2021
>Accepted Date : 13 October, 2021
>Published Date : 16 October, 2021
>DOI : https://doi.org/10.54289/JOP2100102
>Citation : Olufade O, Yoo A, Negron G, McDermott H, Jayanthi N, et al. (2021). Greater Trochanteric Pain Syndrome (GTPS): A clinical prospective study of treatment options. J Orthop Pract 1(1). doi https://doi.org/10.54289/JOP2100102
>Copyright : © 2021 Olufade O, Yoo A, Negron G, McDermott H, Jayanthi N, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Research Article | Open Access | Full Text
1Emory University School of Medicine, Department of Orthopedics
2Emory Sports Medicine Center
3Emory University School of Medicine, Department of Physical Medicine and Rehabilitation
4University of Alabama School of Medicine
5Emory University School of Medicine, Department of Family and Preventative Medicine
6Emory University, Rollins School of Public Health
*Corresponding author: Oluseun Olufade, Assistant Professor, Department of Orthopedics, Emory School of Medicine, Georgia, US
Abstract
Background: There are few prospective studies evaluating the efficacy of various non-operative strategies for treatment of greater trochanter pain syndrome (GTPS). There is a diversity of available interventions and lack of clear consensus for the best modality thus far.
Design: Observational prospective cohort study performed during the period of October 2017 and March 2019.
Methods: The main objective was to determine if there is a difference in outcome of the Lower Extremity Functional Scale (LEFS) for subjects treated with conservative management (PT), corticosteroid injection (CSI), or percutaneous ultrasonic tenotomy (PUT). Participants were assigned based on physician treatment in a non-randomized manner to PT, a single CSI, or the PUT treatment arm. Subjects participated in outcome assessments at baseline and at 1-, 3-, 6-, and 12-months post intervention.
Results: 112 individuals with unilateral GTPS were recruited for this study with 69 PT patients, 31 CSI patients, and 12 PUT patients. The adjusted mean LEFS scores averaged across all time periods remained statistically different between PT, CSI, and PUT (p = 0.0093), indicating significant difference between each treatment arm. PT group saw the greatest improvements from baseline score starting at 1 month and up to 1 year (p = .0004). CSI group did not see significant LEFS improvement until 6 months (p = 0.04) and did not maintain clinically significant improvement by 1 year. PUT group saw significant LEFS improvement at 3 months (p = 0.0001) and maintained clinically significant improvements (≥ 9 LEFS points) throughout the course of the study.
Conclusion: PT patients over the study period showed the greatest improvements in LEFS scores compared to CSI and PUT patients. We believe that PT is the best indicated course of treatment for GTPS. PUT may be considered as an additional option if patients have failed other treatment modalities. CSI shows benefit at 6 months, but overall inferior to PT and PUT.
Keywords: Gluteal tendinopathy, greater trochanteric pain syndrome, physical therapy, ultrasound, percutaneous tenotomy, musculoskeletal conditions
Abbreviations: GTPS: Greater Trochanteric Pain Syndrome, PRP: platelet rich plasma, LR-PRP: leukocyte-rich PRP, LEFS: Lower Extremity Functional Scale, PT: conservative management, CSI: corticosteroid injection, PUT: percutaneous ultrasonic tenotomy, PUT: percutaneous ultrasonic tenotomy
Introduction
Lateral hip pain, also referred to as Greater Trochanteric Pain Syndrome (GTPS), is a common diagnosis with a litany of possible pathologies ranging from hip bursitis, gluteus tendinopathies, external snapping syndrome, and iliotibial band syndrome. There are other pathologies associated with GTPS including intra-articular hip pain, pain post total hip arthroplasty, and lumbar radiculopathy [1-5]. GTPS has been reported in up to 10 % - 25 % of the population [6].
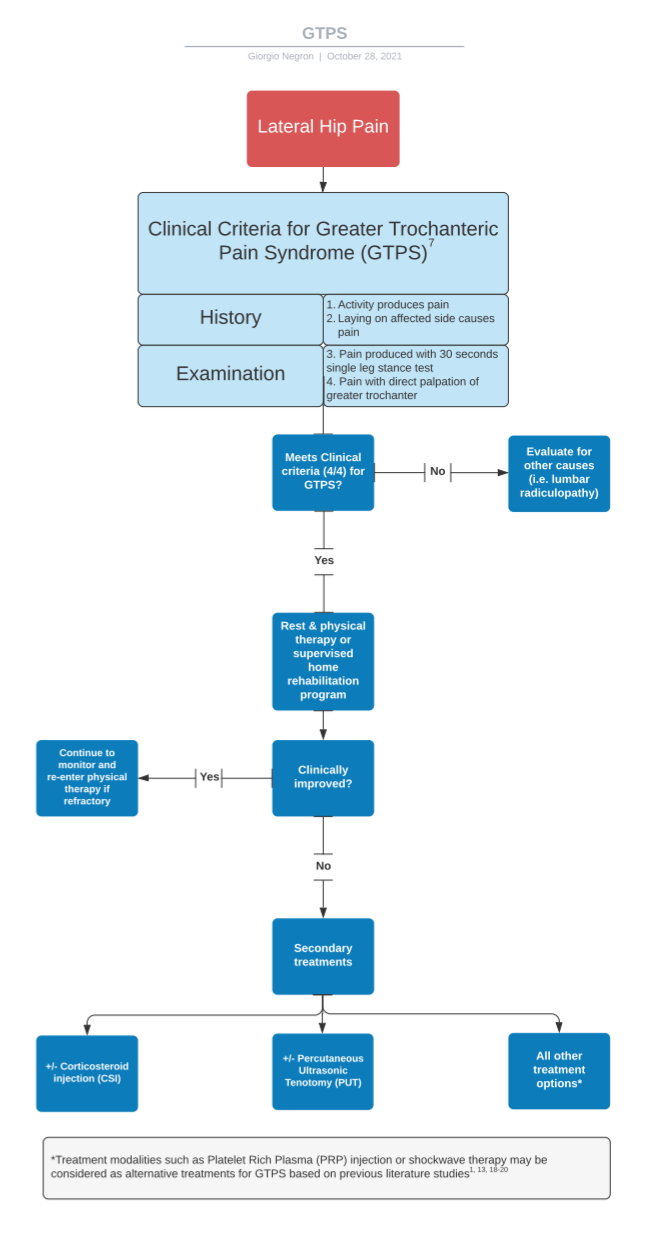
Though a single test for GTPS is typically not enough for clinical judgment, a combination of history and physical examination maneuvers can lead a clinician to a clearer diagnosis [7]. Patients commonly complain of pain on the lateral hip especially when laying on the affected side. Many who are diagnosed with GTPS will be tender to palpation at the symptomatic trochanteric bursa which carries a positive predictive value (PPV) of 83 % [8]. Additionally, symptoms include pain with hip abduction against resistance, pain with single leg stance, a positive Patrick’s, or Ober's test. If a gluteus medius or minimus tear is present, people will often present with weakness and pain with active, resisted hip abduction in extension and external rotation while the hip is flexed to 90 degrees. Though it is not required for the diagnosis of trochanteric bursitis and tendinopathy, plain radiographs are often obtained to evaluate for enthesopathy, calcifications and an intra-articular source of pain. Ultrasound and MRI are the modalities for investigation of gluteus muscle tendonitis or tear [3,5]. Proximal iliotibial band thickness has been correlated with recalcitrant greater trochanteric pain syndrome [9].
Given the array of causes for GTPS, there are several modes of treatment intervention. They range from conservative management with anti-inflammatory medications, rest, weight loss, and physical therapy, to minimally invasive procedures including corticosteroid injections, percutaneous tenotomy, platelet-rich plasma, to surgical intervention for the most severe cases. GTPS is often self-limiting. Trochanteric bursitis is one of the most common diagnoses given for lateral hip pain, but it has been suggested that lateral hip pain is not usually associated with inflammation of the bursa and gluteus medius insertion. Board et al. found that post-op biopsy of the bursa did not always show markers of inflammation [10]. Though many clinicians start with physical therapy or a home-exercise program for treatment of GTPS, a 2017 systematic review demonstrated a sparse amount of high-quality research for conservative management of GTPS. Only until recently, have there been two randomized controlled trials (RCTs) that highlighted that an exercise program may be considered effective for non-surgical management of GTPS [11,12].
Moreover, local anesthetic injections with corticosteroid have had a 77.1 % efficacy rate for 1 week and up to 61.3 % for up to 6 months [13]. Cohen found no difference between fluoroscopic guided injection and bedside injection [6]. Low energy shock-wave therapy has been found to be superior to other non-operative modalities [10,14]. In fact, shock-wave therapy allowed 64 %-76 % of patients to return to normal activities. For re-occurring and refractory cases of GTPS, surgical intervention such as bursectomy and ITB release has been found to be effective [13].
Several retrospective studies have been done to explore the effectiveness of one procedure versus another, such as percutaneous tenotomy vs platelet rich plasma (PRP), but very few prospective studies are available that measure the effectiveness of the treatments. Corticosteroid injection has been known to last for 3-6 months but no significant difference was found when evaluated at 12 months when compared to conservative management [15,16]. Interestingly, the GLUTEAL trial compared CSI vs injection of normal saline and demonstrated no difference between the two for pain relief at 1 and 6 months [17]. Likewise, Rompe et al. found that after one-month shockwave and conservative therapy were superior to CSI [18]. A few small studies have demonstrated effectiveness in pain relief using PRP in the treatment recalcitrant GTPS [1,19,20]. Jacobson et al. first found improvement to gluteal fenestration through retrospective analysis, and later demonstrated an improvement in pain scores to patients in both treatment arms blinded to PRP or gluteal tendon fenestration at 1 and 2 weeks [20,21]. Moreover, a recent study by Fitzpatrick et al. compared a single leukocyte-rich PRP (LR-PRP) injection versus a single CSI for gluteal tendinopathy portraying clinically and statistically significant improvement in pain and hip function at 12 weeks [22]. This was later continued with a 2 year follow up of these patients which showed continued improvement in the LR-PRP group versus CSI group which did not maintain improvement beyond 24 weeks [23].
Percutaneous ultrasonic tenotomy (PUT) is another emerging percutaneous technique which has been utilized for multiple musculoskeletal injuries such as in lateral epicondylitis [24,25], patellar tendinitis [26], Achilles tendinitis [27,28], and plantar fasciitis [28]. Unlike the traditional percutaneous tenotomy procedure requiring manual passes of a needle to abnormal parts of a tendon, PUT utilizes high frequency energy to a needle-like device that removes disease tendon tissue and is subsequently removed by an inflow-outflow fluid circuit. It is thought that through the removal of pathologic disease, this allows a chronic degenerative process to be converted to an acute process [29] In addition, this acute inflammatory condition may introduces growth factors to promote healing [30].
Given the diversity of available interventions, emerging technologies, and lack of clear consensus for the best modality thus far, the researchers believe that identifying the best treatment by diagnosis could have greater positive outcomes for patients through quicker recovery as well as an increase cost savings. Prior research studies have not evaluated these 3 treatment modalities (PT/CSI/PUT) for GTPS in one prospective study. The aim of this study was to determine if there was a difference in outcome using the Lower Extremity Functional Scale (LEFS) for subjects treated with conservative management (PT), corticosteroid injection (CSI), or percutaneous ultrasonic tenotomy (PUT). We hypothesize that physical
120 therapy will show significant improvement in LEFS compared to all treatment modalities. In addition, we hypothesize that PUT would be an effective treatment for refractory GTPS providing an alternative for patients who fail conservative management.
Methods
Study Design:
The Institutional Review Board approval was obtained prior to initiation of this study. This was an observational prospective cohort study of 112 subjects with refractory unilateral greater trochanteric pain syndrome recruited between October 2017 to March 2019. The main objective was to determine if there is a difference in outcome of the Lower Extremity Functional Scale (LEFS) for subjects treated with conservative management (PT), corticosteroid injection (CSI), or percutaneous ultrasonic tenotomy (PUT).
Patients:
Participants were assigned based on physician treatment in a non-randomized manner: 69 PT patients (40 participants chose to pursue a formal course of physical therapy and 29 patients chose the home exercise program), 31 CSI patients, and 12 PUT patients. Subjects participated in outcome assessments at baseline and at 1-, 3-, 6-, and 12-months post-intervention.
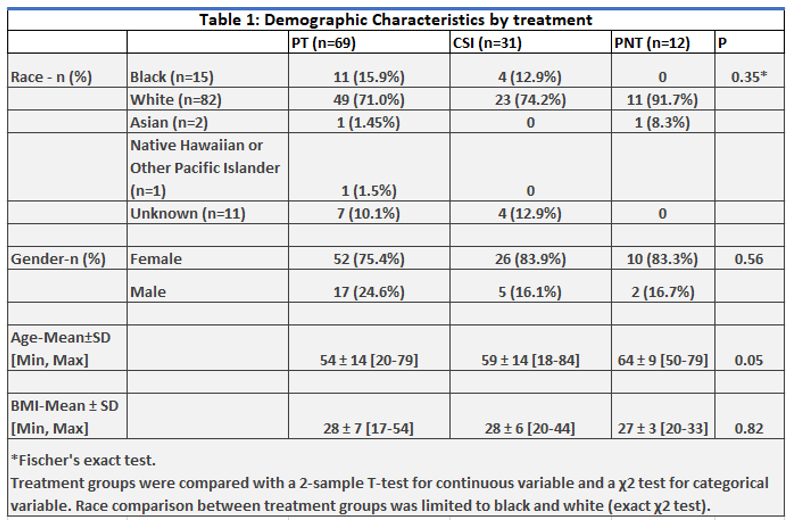
The surveys were examined for any statistically significant difference by race, gender, age, and BMI andfound no statistically significant differences with regard to race (p = 0.35), gender (p = 0.56), age (p = 0.05), and BMI (p = 0.82), respectively (Table 1). Scores were then adjusted based on gender, age, and race (Black and White only).
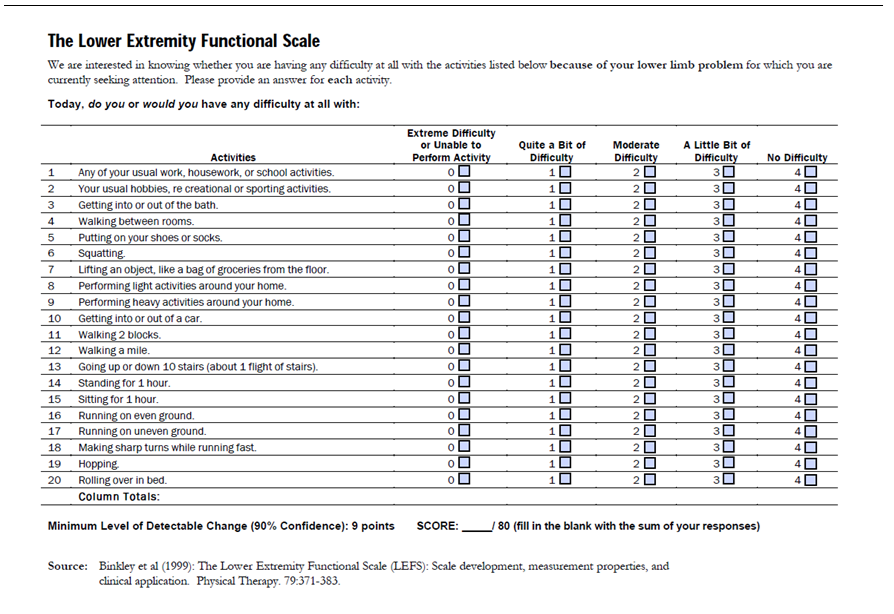
Figure 1: Lower Extremity Functional Scale (LEFS).
In clusion criteria were ages between 18 and 80 who presented to a tertiary Sports Medicine clinic with lateral hip pain. Participants’ symptoms had to be present with resisted hip abduction in the lateral decubitus position and have tenderness with palpation at the greater trochanter. Subjects were excluded if they were under guardianship or with limited cognitive ability that would preclude understanding the questionnaire, had undergone previous hip surgery, had a history of cancer, radiographic evidence of moderate to severe hip osteoarthritis, symptomatic lumbar stenosis, or femoral acetabular impingement.
Subjects were screened by one of two Sports Medicine fellowship-trained physicians for inclusion criteria at the initial clinic visit. Consent was then obtained to participate in the GTPS and a baseline Lower
Extremity Functional Scale (LEFS) was completed in clinic.
Procedures:
Primary outcome measures were assessed using the Lower Extremity Functional Scale (LEFS) [31,32]. The LEFS is a 20-question survey that quantifies the ability to perform everyday tasks. The survey asks patients to quantify the level of difficulty involved in performing 20 everyday activities ranging from putting on shoes to walking various distances. Patients rate each activity using a score from 0 (Extremely difficult/unable to perform) to 4 (No difficulty). Then the scores from each activity are summed to reach a total score, with the maximum score being 80. Lower scores indicate a greater level of overall disability. When comparing between survey time points, the minimal detectable change and minimal clinically detectable significance in this scale is 9 points. The sensitivity and specificity for the LEFS are 0.81 and 0.70, respectively. While various studies used different measurements such, the LEFS survey was designed and validated as a means to evaluate functional impairment and monitor the effectiveness of an intervention over the course of time.[31] Procedures were performed at a single tertiary care center by the two providers who completed the initial screening process. Follow up LEFS were then sent at 1 month, 3 months, 6 months, and 1 year follow ups.
Our initial goal was to recruit 52 non-randomized subjects to each arm: conservative management (PT), a single local corticosteroid injection, or PUT. Conservative management consisted of either formal physical therapy or home exercise program combined with rest, NSAID use, or a combination of the subjects’ choosing, no guidance given for course to pursue. Participants who underwent formal physical therapy received a prescription focusing on isometric loading of the gluteus medius and minimus with progression to functional isotonic exercises. Prescription duration was set for 6 weeks with a frequency of two to three times week.
Alternatively, a home exercise program was given with isotonic exercises and incorporation of lateral hip exercises (i.e., lateral kicks, clamshells, and band walks). Direction and pictures were included with suggested routine of 10 repetition with each leg for 3 sets daily.
For the CSI group, half of the patients had usual care which may have included supervised or formal rehabilitation, while the other half had no prior therapy. Patients were given either an injection of 1 ml of methylprednisolone acetate (40 mg/ml) or triamcinolone acetonide (40 mg/ml) mixed with 1 ml of 1 % lidocaine and 1 ml of normal saline. Sterile technique was used, and the injection was done under ultrasound guidance to the peri-trochanteric space.
As for the PUT treatment arm, all patients had tried and previously underwent conservative management including PT and CSI. For procedural care, the patient’s skin surface was first prepared with antimicrobial solution and draped in a sterile fashion. The provider then injected 10 ml of 1 % lidocaine for local anesthetic above the gluteus medius and minimus tendons. An #11 blade was used to incise through the skin which facilitated entry for the tip of percutaneous tenotomy instrument (Tenex TX System) and advanced with ultrasound guidance. The tendons were treated with ultrasonic energy and following the procedure, steri-strips were placed to close the incision.
Statistical Analysis
A repeated-measures analysis of lower extremely functional scale was performed with a means model via the SAS MIXED Procedure (version 9.4; SAS Institute, Cary, NC), providing separate estimates of mean LEFS by time on study (baseline, 1,3,6, and 12 months) and treatment group (PT, CSI and PUT). The model included three predictors (treatment arm, time on study [categorical clinical visit] and the statistical interaction between treatment arm and time on study). A compound-symmetric variance-covariance form in repeated measurements was assumed for LEFS and robust estimates of the standard errors of parameters were used to perform statistical tests and construct 95 % confidence intervals. The model-based means are unbiased with unbalanced and missing data, as long as the missing data are non-informative (missing at random). A P-value ≤ 0.05 was considered statistically significant for the main effects (treatment and time on study) and for the treatment by time on study interaction effect from the repeated-measures analysis. The minimal clinically significant difference of a change in 9 points on the LEFS was round up to the nearest integer. The statistical test for interaction between time on study and treatment was the overall hypothesis test to determine whether LEFS demonstrated different patterns over time by treatment group (i.e., different temporal patterns over time). Since mean LEFS in the three treatment groups was consistently different over time (i.e., no statistical interaction) then the main effect test for treatment was used as the primary hypothesis test to compare the 3 treatment groups (time-averaged treatment means). The primary study results from this model include the mean LEFS and 95 % confidence interval for the PT group, the mean LEFS and 95 % confidence interval for the CSI group and the mean LEFS and 95 % confidence interval for the PUT group. Specific statistical tests were done within the framework of the mixed effects linear model. All statistical tests were 2-sided and unadjusted for multiple comparisons. The repeated-measures model was refitted to adjust for gender, race and age at enrollment. The percentage change from baseline LEFS was analyzed using the same analysis plan described for lower extremity functional scale scores.
Results:
Time Averaged Mean Scores:
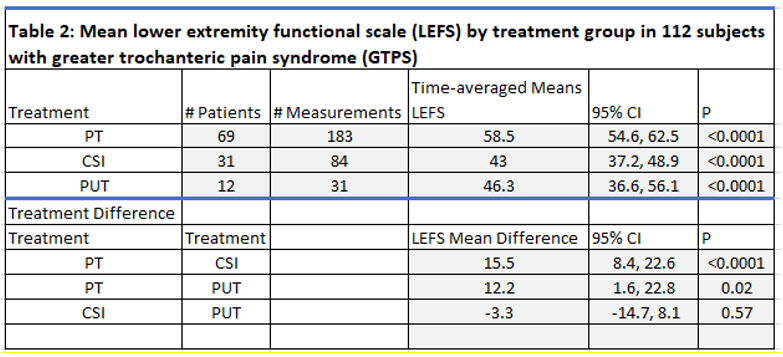
The time averaged mean LEFS scores (Table 2), which were the mean scores over the course of 1 year, were statistically different between each treatment arm with PT, CSI, and PUT scores reporting 58.5, 43, and 46.3, respectively (p < .0001).
This was to show that there were significant differences overall between the 3 treatment groups.
PT vs CSI
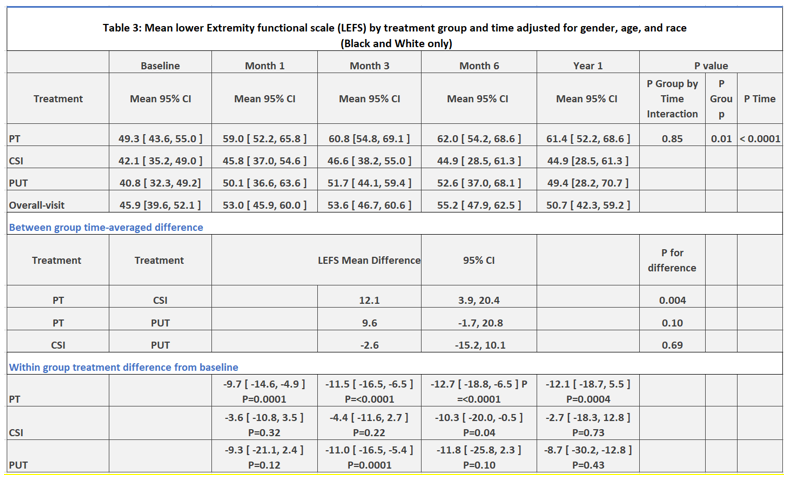
The PT arm saw mean differences with CSI and PUT that were clinically significant (≥ 9 LEFS points) over the study period. PT vs CSI saw a mean LEFS difference of 15.5 (p < 0.0001) (Table 2). When looked across time (Table 3), PT patients saw the greatest improvements from baseline score throughout the course of the study starting at 1 month with conservative management and up to 1 year (p = .0004). CSI did not see significant LEFS improvement until 6 months (p = 0.04) and did not maintain clinically significant improvement by 1 year.
PT vs PUT
PT vs PUT saw a mean LEFS difference of 12.2 (p = 0.02) (Table 2). When looked across time, PUT saw significant LEFS improvement at 3 months (p = 0.0001) and maintained clinically significant improvements throughout the course of the study. Whereas PT saw clinically significant improvements starting at 1 month and maintained improvements throughout the course of the study.
CSI vs PUT
CSI vs PUT showed there was no difference between the 2 arms with a mean LEFS difference of -3.3 (p = 0.57) (Table 2). As stated previously, PUT saw significant improvements by 3 months and maintained clinically significant improvements, while CSI did not show improvements till 6 months and did not maintain clinically significant improvements by the end of the study period.
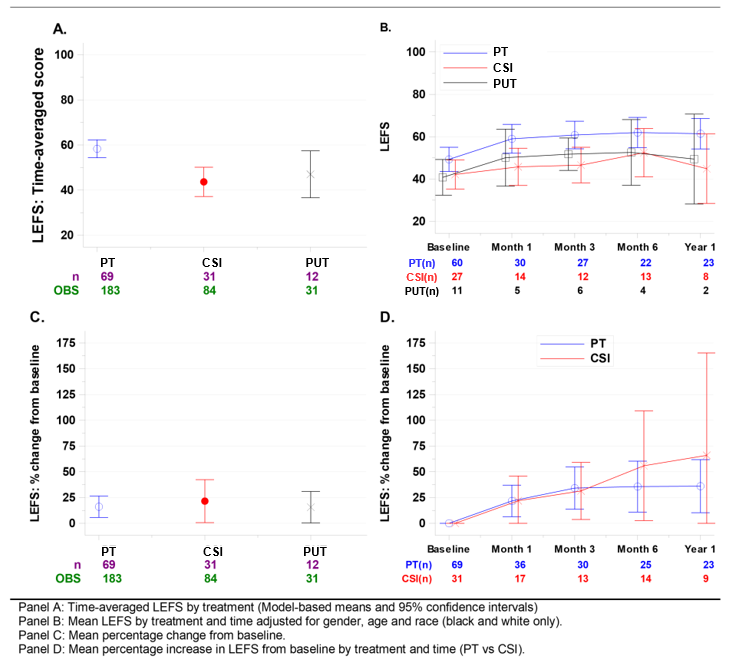
Figure 2: highlights graphs of data analysis.
Discussion:
Prior research studies have not evaluated these 3 treatment modalities (PT/CSI/PUT) for GTPS in one prospective study. Also, prior studies have not used the same assessment tool to compare these various treatment modalities. For example, in the Jacobson et al. study, customized pain scores were used to compare outcomes of PUT vs PRP treatment [20].
In the GLUTEAL trial, a numerical rating scale (NRS) pain score was used to measure outcomes for a CSI [17]. This study used one assessment tool (LEFS) to compare all 3 treatment arms. By comparing these treatment modalities using the same assessment tool (LEFS), this prospective observational study provides a new layer to the treatment algorithm for GTPS (Figure 2). This study showed consistency with previous retrospective studies [16-18], demonstrating limited functional and pain improvement from GTPS with a corticosteroid injection in comparison to conservative treatment, such as physical therapy or rest.
Physical Therapy/Conservative Management
GTPS is believed to be a multifactorial chronic form of tendinopathy arising from repetitive microtrauma involving the gluteal tendons at the level of the greater trochanter. One of the biggest factors contributing to the etiology of GTPS appears to be mechanical overload and pelvic biomechanics [33]. The pathophysiology of this chronic microtrauma is believed to ultimately lead to inflammation and degeneration of the tendons via disruption of the collagen matrix with neovascularization and increased protein synthesis leading to scar tissue and chronic inflammation [34].
In this study, patients treated with physical therapy made the greatest improvements based on the LEFS. Over the study period, physical therapy continued to show the greatest improvement clinically and was statistically significant throughout the entire course of 1 year. This is supported with clinical evidence that patients in this population usually lack hip abductor strength seen in single leg stance and gait which physical therapy and home training can assist with addressing the underlying pathology [35-38].
Recently, two randomized controlled trials highlighted the use of exercises regimens for GTPS. Mellor et al. created a three-arm prospective randomized controlled trial for patients with lateral hip pain, including load management exercise with education on tendon loading, a CSI group, and a wait and see approach. It was found that CSI provided global improvement (function and quality of life) in the short term (8 weeks) but in the long term (52 weeks), the exercise and education group had better overall global improvement [12]. In addition, Ganderton et al. randomized participants to receive either to the GLoBE protocol (Luteal La Trope University exercise program) or sham exercise (seated exercise). Both groups received an educational booklet on reducing tendon load. Though there was an improvement in pain and function in both groups at 12 and 52 weeks with no significant difference, the GloBE group improved to a greater degree [11].
A recent literature review of evidence-based treatments for GTPS also found that activity modification and physical therapy also appeared to provide benefits. It was found that activity modifications by means of reducing compression and overload on tendons was recommended. These included avoiding aggravating activities such as climbing stairs or walking on irregular surfaces as well as static positional activities such as lying on the affected sides or positions where the hip is adducted while sitting. The review also found that exercises that focused on retraining hip abductors and dynamic control during adduction appeared to provide effective treatment. Additionally, exercise programs that focus on isometric and isotonic exercises seemed to be the most beneficial [39].
CSI
In this study, patients treated with corticosteroid injections did improve over time, but not as significant as patients treated with physical therapy. Half of the patients in the CSI arm had done some form of PT or injection in the past without improvement. Based on the results, CSI patients did appear to achieve temporary pain relief and increase in function by 6 months. However, these improvements were not maintained by 1 year. This follows with the study by Brinks et al. that also showed temporary pain relief by 3 months, but no differences in outcome by 1 year compared to conservative management [16]. This also follows along with other studies that have used CSI in the short term to treat pain associated with lateral epicondylitis and rotator cuff injuries [40,41]. It should be considered that CSI may not be a well indicated long term therapy for GTPS due to CSI mainly working to reduce more acute inflammatory processes whereas GTPS is a more chronic process. Furthermore, it should be considered that the physical act of introducing a needle into the affected area could provide minor mechanical release of scar tissue and adhesions as well as recruiting local acute inflammatory factors to promote healing and revascularization, which ultimately contributes to the short-term relief of symptoms [41].
PUT
Similarly, patients in the PUT arm also saw improvements over time, but not as significantly as those in the PT arm. All patients in the PUT arm had done some form of PT or injection in the past without improvement.
The theory of PUT, is to debride chronic tendon pathology. As mentioned before, the physical act of introducing a needle to release scar tissue and promote local healing factors is the basis of using PUT to debride, drain, and promote acute inflammation in order to recruit local healing factors and revascularization [34,41].
To our knowledge, there is only one prospective case series that demonstrated the use of PUT for GTPS. Baker et al. followed 29 patients who failed conversative management for gluteal tendinopathy for up to 30 months post-PUT. Results showed significant improvement in VAS scores, Harris Hip scores, and SF-12 scores. There were no complications, however, three patients eventually ended up proceeding to hip abductor tendon repair [42]. This study, along with ours supports the clinical use of PUT for potential treatment of GTPS.
PUT, while a limited number of subjects, showed sustained clinically significant LEFS improvement (≥ 9 LEFS points) at three months. With that said, the effect of PUT may not have been as long-lasting, likely due to the severity of condition (all PUT patients had failed other treatments such as CSI or PT) and other potential silent pathologies such as lumbar radiculopathy. This is similar to prior studies done by Jacobson et al., which showed marked improvements in patients who received tendon fenestration20,21. Similarly, to CSI, it should be considered that the mechanical release and drainage of inflammatory and calcified tissues may help to treat the underlying causes of GTPS. However, PUT provides a more thorough mechanical treatment of the affected areas compared to CSI which is a single shot. Overall, PUT may be a viable interventional treatment for gluteus medius and gluteus minimus tendinopathy for patients that did not get better with physical therapy and corticosteroid injection.
We recommend that the treatment algorithm (Figure 3) for Greater Trochanteric Pain Syndrome (GTPS) should include conservative management such as rest, NSAIDs, and PT (home exercise or formal) as the first line therapy. Secondary potential options may include percutaneous ultrasonic tenotomy (PUT) for patients who have failed other treatment modalities. Other modalities that show promising results in prior research studies discussed earlier (i.e., PRP treatment and shockwave therapy) were not directly studied in this particular study but can be considered as additional options. [1,13,18-20]. We recognize providers will use corticosteroid injections based on adherence of a traditional treatment but based on our data PUT may be better indicated long term.
Limitations
We acknowledge several limitations to this study. Given the nature of non-incentivized studies followed over a long time period (1 year), the participant non-response rate ranged from 31 % -54 %. The survey non-response rate for 1 month, 3 month, 6 month, and 1 year follow ups, were 54 %, 46 %, 41 %, and 31 %, respectively. The overall dropout rate for the total study was 32 %, when looking at participants that never filled out a follow up survey after the baseline survey and 68 % of participants filling out at least one follow up survey. Also, there were a limited number of patients eligible to be recruited in the PUT treatment arm (n = 12). While the purpose was to participate with non-uniform conservative managements already in practice, the variability of participants’ conservative management could have influenced differences of LEFS outcomes for this baseline arm. Additionally, this study was an observational study and thus not a blinded randomized controlled trial with uniform randomization. Such a study would help provide additional important information.
Conclusion:
Overall, we believe that PT is the best indicated course of treatment for GTPS. PUT may be considered as an additional option if patients have failed other treatment modalities. CSI shows benefit at 6 months, but overall inferior to PT and PUT.
Acknowledgements: None
Conflict of Interest: None
References
- Lee JJ, Harrison JR, Boachie-Adjei K, Vargas E, Moley PJ. (2016) Platelet-Rich Plasma Injections With Needle Tenotomy for Gluteus Medius Tendinopathy: A Registry Study With Prospective Follow-up. Orthop J Sports Med. 4(11): 2325967116671692. [PubMed.]
- Capogna BM, Shenoy K, Youm T, Stuchin SA. (2017) Tendon Disorders After Total Hip Arthroplasty: Evaluation and Management. J Arthroplasty. 32(10): 3249-3255. [PubMed]
- Lequesne M, Djian P, Vuillemin V, Mathieu P. (2008) Prospective study of refractory greater trochanter pain syndrome. MRI findings of gluteal tendon tears seen at surgery. Clinical and MRI results of tendon repair. Joint Bone Spine. 75(4): 458-464. [PubMed.]
- Williams BS, Cohen SP. (2009) Greater trochanteric pain syndrome: a review of anatomy, diagnosis and treatment. Anesth Analg.108(5): 1662-1670. [PubMed.]
- Shemesh SS, Moucha CS, Keswani A, Maher NA, Chen D,et al. (2018) Trochanteric Bursitis Following Primary Total Hip Arthroplasty: Incidence, Predictors, and Treatment. J Arthroplasty. 33(4): 1205-1209. [PubMed.]
- Cohen SP, Strassels SA, Foster L, et al. (2009) Comparison of fluoroscopically guided and blind corticosteroid injections for greater trochanteric pain syndrome: multicentre randomised controlled trial. BMJ. 338: b1088. [Ref.]
- Speers CJ, Bhogal GS. (2017) Greater trochanteric pain syndrome: a review of diagnosis and management in general practice. Br J Gen Pract. 67(663): 479-480. [Ref.]
- Grimaldi A, Mellor R, Nicolson P, Hodges P, Bennell K,et al. (2017) Utility of clinical tests to diagnose MRI-confirmed gluteal tendinopathy in patients presenting with lateral hip pain. British Journal of Sports Medicine. 51(6): 519-524. [PubMed.]
- Khoury AN, Brooke K, Helal A, et al. (2018) Proximal iliotibial band thickness as a cause for recalcitrant greater trochanteric pain syndrome. J Hip Preserv Surg 5(3): 296-300. [Ref.]
- Board TN, Hughes SJ, Freemont AJ. (2014) Trochanteric bursitis: the last great misnomer. Hip Int. 24(6): 610-615. [Ref.]
- Ganderton C, Semciw A, Cook J, Moreira E, Pizzari T. (2018) Gluteal Loading Versus Sham Exercises to Improve Pain and Dysfunction in Postmenopausal Women with Greater Trochanteric Pain Syndrome: A Randomized Controlled Trial. J Womens Health (Larchmt). 27(6): 815-829. [PubMed.]
- Mellor R, Bennell K, Grimaldi A, et al. (2018) Education plus exercise versus corticosteroid injection use versus a wait and see approach on global outcome and pain from gluteal tendinopathy: prospective, single blinded, randomised clinical trial. Br J Sports Med. 52(22): 1464-1472. [Ref.]
- Lustenberger DP, Ng VY, Best TM, Ellis TJ. (2011) Efficacy of treatment of trochanteric bursitis: a systematic review. Clin J Sport Med. 21(5): 447-453. [PubMed.]
- Torres A, Fernandez-Fairen M, Sueiro-Fernandez J. (2018) Greater trochanteric pain syndrome and gluteus medius and minimus tendinosis: nonsurgical treatment. Pain Manag. 8(1): 45-55. [PubMed.]
- Koulischer S, Callewier A, Zorman D. (2017) Management of greater trochanteric pain syndrome : a systematic review. Acta Orthop Belg. 83(2): 205-214. [PubMed.]
- Brinks A, van Rijn RM, Bohnen AM, et al. (2007) Effect of corticosteroid injection for trochanter pain syndrome: design of a randomised clinical trial in general practice. BMC Musculoskelet Disord. 8: 95. [PubMed.]
- Nissen MJ, Brulhart L, Faundez A, Finckh A, Courvoisier DS,et al. (2019) Glucocorticoid injections for greater trochanteric pain syndrome: a randomised double-blind placebo-controlled (GLUTEAL) trial. Clin Rheumatol. 38(3): 647-655. [PubMed.]
- Rompe JD, Segal NA, Cacchio A, Furia JP, Morral A, et al. (2009) Home training, local corticosteroid injection, or radial shock wave therapy for greater trochanter pain syndrome. Am J Sports Med. 37(10): 1981-1990. [PubMed.]
- Mautner K, Colberg RE, Malanga G, et al. (2013) Outcomes after ultrasound-guided platelet-rich plasma injections for chronic tendinopathy: a multicenter, retrospective review. PM R. 5(3): 169-175. [PubMed.]
- Jacobson JA, Yablon CM, Henning PT, et al. (2016) Greater Trochanteric Pain Syndrome: Percutaneous Tendon Fenestration Versus Platelet-Rich Plasma Injection for Treatment of Gluteal Tendinosis. J Ultrasound Med. 35(11): 2413-2420. [PubMed.]
- Jacobson JA, Rubin J, Yablon CM, Kim SM, Kalume-Brigido M, et al. (2015) Ultrasound-Guided Fenestration of Tendons About the Hip and Pelvis: Clinical Outcomes. J Ultrasound Med. 34(11): 2029-2035. [PubMed.]
- Fitzpatrick J, Bulsara MK, O'Donnell J, McCrory PR, Zheng MH. (2018) The Effectiveness of Platelet-Rich Plasma Injections in Gluteal Tendinopathy: A Randomized, Double-Blind Controlled Trial Comparing a Single Platelet-Rich Plasma Injection With a Single Corticosteroid Injection. Am J Sports Med. 46(4): 933-939. [PubMed.]
- Fitzpatrick J, Bulsara MK, O'Donnell J, Zheng MH. (2019) Leucocyte-Rich Platelet-Rich Plasma Treatment of Gluteus Medius and Minimus Tendinopathy: A Double-Blind Randomized Controlled Trial With 2-Year Follow-up. Am J Sports Med. 47(5): 1130-1137. [PubMed.]
- Barnes DE, Beckley JM, Smith J. (2015) Percutaneous ultrasonic tenotomy for chronic elbow tendinosis: a prospective study. J Shoulder Elbow Surg. 24(1): 67-73. [PubMed.]
- Seng C, Mohan PC, Koh SB, et al. (2016) Ultrasonic Percutaneous Tenotomy for Recalcitrant Lateral Elbow Tendinopathy: Sustainability and Sonographic Progression at 3 Years. Am J Sports Med. 44(2): 504-510. [PubMed.]
- Nanos KN, Malanga GA. (2015) Treatment of Patellar Tendinopathy Refractory to Surgical Management Using Percutaneous Ultrasonic Tenotomy and Platelet-Rich Plasma Injection: A Case Presentation. Pm r. 7(12): 1300-1305. [PubMed.]
- Chimenti RL, Stover DW, Fick BS, Hall MM. (2019) Percutaneous Ultrasonic Tenotomy Reduces Insertional Achilles Tendinopathy Pain With High Patient Satisfaction and a Low Complication Rate. J Ultrasound Med. 38(6): 1629-1635. [PubMed.]
- Langer PR. (2015) Two emerging technologies for Achilles tendinopathy and plantar fasciopathy. Clin Podiatr Med Surg. 32(2): 183-193. [PubMed.]
- Jacobson JA, Kim SM, Brigido MK. (2016) Ultrasound-Guided Percutaneous Tenotomy. Semin Musculoskelet Radiol. 20(5): 414-421. [PubMed.]
- Chiavaras MM, Jacobson JA. (2013) Ultrasound-guided tendon fenestration. Semin Musculoskelet Radiol. 17(1): 85-90. [PubMed.]
- Binkley JM, Stratford PW, Lott SA, Riddle DL. (1999) The Lower Extremity Functional Scale (LEFS): scale development, measurement properties, and clinical application. North American Orthopaedic Rehabilitation Research Network. Phys Ther. 79(4): 371-383. [PubMed.]
- Dingemans SA, Kleipool SC, Mulders MAM, et al. (2017) Normative data for the lower extremity functional scale (LEFS). Acta Orthop. 88(4): 422-426. [PubMed.]
- Reid D. (2016) The management of greater trochanteric pain syndrome: A systematic literature review. J Orthop. 13(1): 15-28. [PubMed.]
- Rees JD, Maffulli N, Cook J. (2009) Management of tendinopathy. Am J Sports Med. 37(9): 1855-1867. [PubMed.]
- Fearon A, Neeman T, Smith P, Scarvell J, Cook J. (2017) Pain, not structural impairments may explain activity limitations in people with gluteal tendinopathy or hip osteoarthritis: A cross sectional study. Gait Posture 52: 237-243. [PubMed.]
- Allison K, Bennell KL, Grimaldi A, Vicenzino B, Wrigley TV,et al. (2016) Single leg stance control in individuals with symptomatic gluteal tendinopathy. Gait Posture. 49: 108-113. [PubMed.]
- Allison K, Wrigley TV, Vicenzino B, Bennell KL, Grimaldi A,et al. (2016) Kinematics and kinetics during walking in individuals with gluteal tendinopathy. Clin Biomech (Bristol, Avon). 32: 56-63. [PubMed.]
- Ganderton C, Pizzari T, Harle T, Cook J, Semciw A. (2017) A comparison of gluteus medius, gluteus minimus and tensor facia latae muscle activation during gait in post-menopausal women with and without greater trochanteric pain syndrome. J Electromyogr Kinesiol. 33: 39-47. [PubMed.]
- Marin-Pena O, Papavasiliou AV, Olivero M, Galanis N, Tey-Pons M,et al. (2020) Non-surgical treatment as the first step to manage peritrochanteric space disorders. Knee Surg Sports Traumatol Arthrosc 2020. [PubMed.]
- Smidt N, van der Windt DA, Assendelft WJ, Deville WL, Korthals-de Bos IB,et al. (2002) Corticosteroid injections, physiotherapy, or a wait-and-see policy for lateral epicondylitis: a randomised controlled trial. Lancet. 359(9307): 657-662. [PubMed.]
- Housner JA, Jacobson JA, Misko R. (2009) Sonographically guided percutaneous needle tenotomy for the treatment of chronic tendinosis. J Ultrasound Med. 28(9): 1187-1192. [PubMed.]
- Baker CL Jr, Mahoney JR. (2020) Ultrasound-Guided Percutaneous Tenotomy for Gluteal Tendinopathy. Orthop J Sports Med 8(3): 2325967120907868. [PubMed.]