>Corresponding Author : Alejandro Alvarez López
>Article Type : Mini Review Article
>Volume : 1 | Issue : 1
>Received Date : 24 September, 2021
>Accepted Date : 10 October, 2021
>Published Date : 14 October, 2021
>DOI : https://doi.org/10.54289/JOP2100101
>Citation : López AA (2021). External fixation in distal radius fractures J Orthop Pract 1(1). doi https://doi.org/10.54289/JOP2100101
>Copyright : © 2021 López AA. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Mini Review Article | Open Access | Full Text
Doctor en Ciencias Médicas. Especialista de Segundo Grado en Ortopedia y Traumatología. Máster en Urgencias Médicas. Profesor Titular. Investigador auxiliar del CITMA. Universidad de Ciencias Médicas. Hospital Universitario Manuel Ascunce Domenech. Departamento de Ortopedia y Traumatología. Camagüey. Cuba
*Corresponding author: Alejandro Alvarez López, MD, PhD, Calle 2 da No 2. Esq. Lanceros. Reparto La Norma. Camagüey Ciudad 1
Abstract
Background: Distal radius fractures are frequent in emergency departments, treatment is generally conservative, but there are patients who meet certain criteria of instability who need surgical treatment, including external fixation.
Aim: To update on the most important elements regarding the use of external fixation in unstable fractures of the distal radius.
Methods: The search and analysis of the information was carried out in a period of 30 days (from April 1 to April 30, 2021) and the following words were used: distal radius fractures, distal radius fractures and external fixation and unstable radius fractures from the information obtained, a bibliographic review of a total of 809 articles published in the PubMed databases, Hinari, SciELO and Medline was carried out using the search manager and EndNote reference manager, of which 44 selected citations were used to perform the review, 37 from the last five years.
Development: The criteria to be taken into account for the instability described by various authors are indicated, as well as the imaging parameters. The two most used classification systems are mentioned. Reference is made to general surgical indications, external fixation, and placement of additional wires. Complications are discussed and a comparison is made between external fixation and blocked volar plates.
Outcome: External fixation in patients with unstable distal radius fracture is a useful treatment option.
Key words: Distal radius fracture; Unstable distal radius fracture; External fixation.
Abbreviations: FDER: Fractures of the distal end of the radius, EF: external fixation
Introduction
Fractures of the distal end of the radius (FDER) are one of the most frequent, according to Egol KA et al. [1] represent one in six fractures treated in emergency services and 16 % of all fractures attended by specialists in Orthopedics and Traumatology. It affects approximately 650,000 people a year in the United States of America.
The female sex is the most affected due to the presence of greater osteoporosis in the fractured area. Below 40 years of age, it has an incidence of 368 per 100,000 and above 40 years the incidence is 1,150 per 100,000 inhabitants. [2,3,4]
FDERs are caused by high-energy trauma in the young patient and low-energy trauma in the elderly caused by axial compression of the limb with the wrist in 40-90 degree extension. In the latter case, bone fragility fractures are considered. [5,6,7]
The clinical picture is characterized by pain, loss of joint mobility, edema, deformity in the back of the fork and bayonet, in addition to the Laugier sign that consists of the location at the same level of the ulnar and radial styloids, which is observed in patients with displaced fractures. [1,8]
Although conservative treatment is the most widely used, there are situations in which surgical intervention is necessary through placement of wires, plates and screws, in addition to external fixation (EF). [9,10]
EF offers multiple advantages due to its relative ease of application, is justified in most fracture patterns, and can be combined with other surgical procedures. [11,12]
Due to the importance of this topic and the large number of patients with this traumatic entity who may need EF, a review of the topic was carried out with the guiding objective of updating on this surgical modality.
Methods
The search and analysis of the information was carried out in a period of 30 days (from April 1 to April 30, 2021) and the following words were used: distal radius fractures, distal radius fractures and external fixation and unstable radius fractures from the information obtained, a bibliographic review of a total of 809 articles published in the databases PubMed [https://pubmed.ncbi.nlm.nih.gov/], Hinari [https://www.who.int/hinari / es /], SciELO [https://scielo.org/es/] and Medline [https://medlineplus.gov/spanish/] through the search manager and reference manager EndNote, of which 44 selected citations were used to perform the review, 37 of the last five years. The words selected for the search were taken from MeSH (Medical Subject Headings). Studies in young and elderly patients were considered. Investigations in patients with poorly consolidated fractures who required EF as a method of correcting deformity treatment were excluded.
Developing
There are conditions in some FDERs, in which conservative treatment cannot be applied, due to initial or secondary displacement, instability, associated injuries, age of the patient and level of physical activity, among others. [13, 14, 15] Instability is one of the most important criteria for defining surgical intervention and the best known are those described by Fernandez DL, LaFontaine M, Cooney WP and Abbaszadegan H cited by Evans BT et al. [16] (table 1).
Table 1: Instability criteria for patients with fractures of the distal end of the radius.
| Author | Criteria |
|---|---|
| Fernandez DL. |
Dorsal comminution greater than 50 % of the radius height in the sagittal plane.
Palmar metaphyseal comminution. Initial dorsal angulation greater than 20 degrees. Initial displacement greater than one centimeter. Initial shortening greater than five millimeters. Intra-articular involvement. Associated ulnar fracture. Severe osteoporosis. |
| LaFontaine M. |
Initial dorsal angulation greater than 20 degrees.
Dorsal metaphyseal comminution. Radiocarpal intra-articular involvement. Associated ulnar fracture. Age over 60 years. |
| Cooney WP. | Dorsal comminution.
Initial dorsal angulation greater than 20 degrees. Extensive intra-articular involvement. |
| Abbaszadegan H. | Shortening or initial impaction greater than four millimeters. |
Plain radiography in anteroposterior and lateral views are helpful in defining fracture patterns. The normal imaging parameters in terms of mean, range, and acceptability of the reduction are shown in Table 2. [17,18,19]
Table 2: Imaging parameters, average, range and acceptable values.
| Parameters | Average/Normal | Range | Acceptable |
|---|---|---|---|
| Radial inclination | 23 (dregrees) | 21-25 (degrees) | Not less than 10 degrees. |
| Radial lenght | 11 (millimeters) | 10-13 (millimeters) | Between two or three millimeters in relation to the contralateral wrist (radius).
Less than five millimeters of shortening. |
| Palmar (volar) tilt | 11-12 (degrees) | 0-20 (degrees) | Zero degree neutral tilt. |
| Intra-articular step | Should not be present. | Not applicable. | Less than two millimeters. |
| Carpal malalignment. | Must not be present. | Not applicable. | Absent. |
| Dorsal angulation. | Must not be present. | Not applicable. | Less than five degrees. |
| Ulnar variance | About two millimeters from the ulnar facet. | No more than two millimeters. | Neutral or negative. |
| Radius width | Must be symmetrical. | Not applicable. | Presence of symmetry. |
The classifications mostly depend on the geometric configuration of the fractures and the most used are those described by Fernandez DL cited by Evans BT et al., [16] who divide fractures into five types, based on the production mechanism; and that of group AO, the A are extra-articular, B partially articular, and C comminuted. There are other classification systems but they are less used, according to Egol KA et al. [1] Although the treatment of this traumatic condition is generally conservative, there are conditions in which it cannot be applied due to displacement, associated injuries, the age of the patient, their level of physical activity, among others. [20, 21, 22] Surgical treatment has several modalities such as the use of Kirschner wires and volar plates. [23, 24] On the other hand, EF, which can be used based on the principle of ligamentotaxis, has multiple advantages, among which are its easy application, it allows to restore the length of the radius, and facilitates the healing of soft tissues in case of open fractures and has a low complication rate. One of the first descriptions of the use of EF was made by Anderson R and O'Neil G in 1944 cited by Simic PM et al. [25] where they used skeletal traction on a simple bar. The general indications for surgical treatment in patients with FEDR are: high-energy trauma, secondary loss of reduction, articular comminution with step off or gap, metaphyseal comminution or bone loss, incongruity of the distal radioulnar joint, open fractures, associated fractures of the carpus, associated tendon and vascular nerve damage, bilateral fractures and affected contralateral limb. [26,27] On the other hand, the specific indications for EF in the wrist are: unstable fractures, patients with acute trauma to the wrist accompanied by dislocation of the carpal bones and the radiocarpal joint, for damage control, in severely comminuted fractures with loss of bone substance in which it is necessary to maintain the length of the radius, open fractures with loss of soft tissues and severe contamination, in addition to the stabilization of the wrist due to infections. [1,28,29] Factors affecting treatment can be local: bone quality, soft tissue damage, comminution, initial displacement of the fracture, and intensity of trauma. From the patient: biological age, lifestyle, occupation, dominant hand, medical conditions and associated damages; as well as the presence of unacceptable radiographic parameters and malalignment of the carpal bones with the distal radius. [1,5] There are two types of EF, those that use the wrist as a bridge and the others that do not. In the first case, it is based on the effect of ligamentotaxis (traction of the bone fragments through the insertions of the ligaments). Bridge-type EF is indicated in patients with an unstable fracture due to extra-articular or articular dorsal comminution with minimal displacement and when the distal fragment is so small that it does not allow wire placement. This type of FE can be static or dynamic. [30,31,32]
On the other hand, the indications for non-bridging EF are: extra-articular unstable fractures or with articular extension reducible by closed methods and at least one centimeter of intact volar cortex is required for the placement of the wires; this requirement is also essential for the use of volar plates and screws. [5,32] To increase stability when using EF, some alternative methods can be used such as the placement of Kirschner wires through the radial and / or ulnar areas of the distal end of the radius, which are cut and bent approximately one centimeter from the skin of the patient. This treatment modality is justified in the case of extra and intra-articular fractures with dorsal angulation, failure of conservative treatment, severe bone comminution, open fractures and in the case of wrist fractures and dislocations. Contraindications of this technique are the volar fractures of Smith and Barton volar, in addition to patients who cannot be followed up by outpatient consultation. [23,26] There are a variety of percutaneous wire fixation techniques associated with EF, all based on the geometric configuration, such as: through radial styloid (Figure 1A), two crossed wires (Figure 1B), intrafocal (Figure 1C), from the ulna to the radius without transfixation of the distal radioulnar joint (Figure 1D), one wire to the styloid and the other to the distal radioulnar joint (Figure 1E) and the placement of multiple wires from the ulna to the radius (Figure 1F). It is preferred to use only one wire in the radial styloid or to associate it with another from the dorsoradial area of the radius. [5,23]
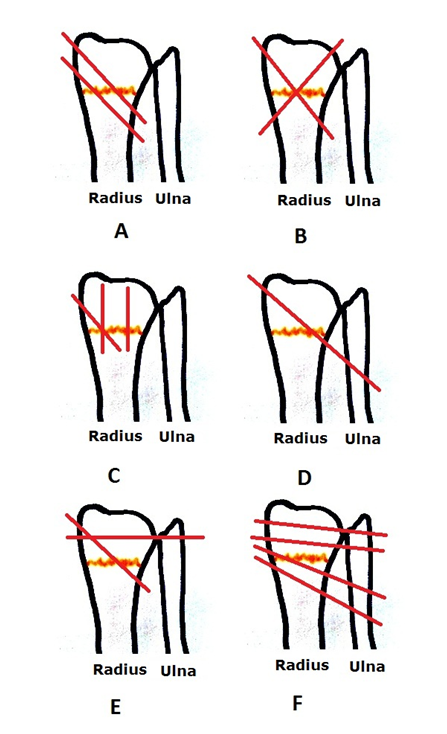
Figure 1: Wire placement associated with external fixation. (Author's own image)
For the placement of the Kirschner wires, the fracture is first reduced, then the wires are placed in the desired position, and then the EF is applied. The wire removal time is six to eight weeks. [1,30] In the presence of impacted fractures in which reduction is not achieved by EF, open reduction by minimal incision, reduction and combination of some internal fixation method is justified. In addition to the combination with open reduction and osteosynthesis, both in the dorsal region and volar as necessary, to achieve anatomical reduction of the fragments. [20, 23, 30] Predictive factors of instability are: age of the patient (patients over 80 years of age have three times more possibilities of re-displacement or instability), degree of initial displacement (especially of the radius), extension of the metaphyseal comminution (greater than one centimeter) and displacement during treatment. [1,5] The complications of EF in patients with FEDR can be divided into three groups, the first attributable to the difficulty to achieve and maintain the reduction of the fracture, the second responds to problems with the wires, and finally the problems of the fracture regardless of the type of treatment such as nerve complications, reflex sympathetic dystrophy, tendon rupture and finger stiffness. [33,34] The problems with the wires are the most frequent complications and among them the infection. Its incidence can be up to 39 % and generally does not interfere with the final result of treatment. Other complications of the wires are breakage and adhesion to the skin, but they occur in only 0.5 to 1 %. [5,34] Currently, there are controversies regarding the superiority of internal fixation with volar plates over EF. However, when analyzing the conclusions of a group of investigations, no criteria were found that affirm this approach in an absolute way in all cases, but there is agreement that the use of volar plates allows earlier rehabilitation and has a higher rate of surgical re-interventions. The long-term functional results between EF and volar plates are very similar according to the authors consulted (Table 3).
Table 3: Comparative elements between EF and internal fixation with volar plate.
| Author | External fixation | Screw-locked plates |
|---|---|---|
| Shukla R et al. [37] | EF is superior in terms of functional results at 1 year compared to internal fixation with volar plates. | |
| Lee DJ et al. [38] | There are no conclusions of superiority between one method or another. Both methods have a good long-term result. | The volar plate is justified in patients who need a quick recovery. |
| Curtin CM et al. [39] | Similar functional results. | Higher rate of re-entry when compared with the FE. |
| Li-Hai Z et al. [40] | Lower incidence of re-operation. Functional results equal at 12 months. | Faster functional result. |
| Bajwa AS et al. [41] | EF is superior in functional results from three months to two years. | |
| Williksen JH et al. [42] | Similar results at five years | Greater need for re-surgical intervention. |
| Chilakamary VK et al. [43] | It is an effective method in unstable fractures, it manages to restore the anatomy and favors rehabilitation. | |
| Ma C et al. [44] | Functional result similar to the year. | Higher incidence of wound infection and re-operation. Better early rehab. |
Conclusion
EF in patients with unstable distal radius fractures is a useful treatment option. For its correct indication, it is necessary to know the instability criteria described, as well as the imaging parameters using plain radiography. The stiffness of external fixation is increased by the use of additional wires in the fractured area. Complications are minimal and the results are similar when compared to screw-locked plates.
References
- Egol KA, Koval KJ, Zuckerman JD. (2020) Handbook of fractures. 6 th ed. Philadelphia: Wolters Kluwer. p.284-295. [Ref.]
- DeGeorge BR Jr, Van Houten HK, Mwangi R, R Sangaralingham L, Kakar S. (2021) Outcomes and complications of operative versus non-operative management of distal radius fractures in adults under 65 years of age. J Hand Surg Eur. 46(2): 159-166. [PubMed]
- Heng BQH, Kang YC, Lim JXY, Chee KG. (2020) Epidemiology of distal radius fixations and functional outcomes in the super elderly population. J Hand Surg Asian Pac Vol. 25(1): 26-31. [PubMed.]
- Rundgren J, Bojan A, Mellstrand Navarro C, Enocson A. (2020) Epidemiology, classification, treatment and mortality of distal radius fractures in adults: an observational study of 23,394 fractures from the national Swedish fracture register. BMC Musculoskelet Disord. 21(1): 88. [PubMed.]
- Zhang F, Yang Y, Zhang H, Luo X. (2020) A comparative study protocol of external fixation versus volar plate in treating distal radius fracture. Medicine (Baltimore). 99(50): e23231. [PubMed.]
- Yan B, Chen Y, Yin W. (2019) Influence of distal radius fractures involving the intermediate column on forearm rotation. J Orthop Surg Res. 14(1): 111. [PubMed.]
- Della Rosa N, Bertozzi N, Adani R. (2020) Biomechanics of external fixator of distal radius fracture, a new approach: Mutifix Wrist. Musculoskelet Surg. [PubMed.]
- Chung KC, Cho HE, Kim Y, Kim HM, Shauver MJ. (2020). Assessment of anatomic restoration of distal radius fractures among older adults: a secondary analysis of a randomized clinical trial. JAMA Netw Open. 3(1): e1919433. [Ref.]
- Carula BC, Pereira MDS, Ferreira APB, Ayzemberg H, Steglich V, et al. (2021) Analysis of the clinical and radiological results of bridge plate versus external fixation in comminuted distal radius fractures. Rev Bras Ortop (Sao Paulo). 56(1): 61-68. [PubMed.]
- Zhou Y, Zhu Y, Zhang X, Tian D, Zhang B. (2019) Comparison of radiographic and functional results of die-punch fracture of distal radius between volar locking plating (VLP) and external fixation (EF). J Orthop Surg Res. 14(1): 373. [Ref.]
- Boydstun S, Nash L, Rayan GM. (2019) Distal radius fracture fixation devices and their radiographs. J Hand Surg Asian Pac Vol. 24(4): 412-420. [PubMed.]
- Curtis DM, Lee CS, Boyajian HH, Lee MJ, Conti Mica M, et al. (2020) Effect of Global Fracture Care Billing on Distal Radius Fractures. Orthopedics. 43(5): e471-e475. [PubMed.]
- Ermutlu C, Mert M, Kovalak E, Kanay E, Obut A, et al. (2020) Management of distal radius fractures: comparison of three methods. 12(8): e9875. [PubMed.]
- Gouk C, Ng SK, Knight M, Bindra R, Thomas M. (2019) Long term outcomes of open reduction internal fixation versus external fixation of distal radius fractures: A meta-analysis. Orthop Rev (Pavia). 11(3): 7809. [PubMed.]
- He B, Tian X, Ji G, Han A. (2020) Comparison of outcomes between nonsurgical and surgical treatment of distal radius fracture: a systematic review update and meta-analysis. Arch Orthop Trauma Surg. 140(8):1143-1153. [Ref.]
- Evans BT, Harper CM, Rozenthal TD. Fractures of the distal radius and ulna. In: Tornetta P, Ricci WM, Ostrum RF, McQueen MM, McKee MD, Court Brown CM. Rockwood and Green's Fractures in Adults. 9 th ed. Philadelphia: Wolters Kluwer; 2020.p.2539-2585. [Ref .]
- Grunz JP, Gietzen CH, Schmitt R, Prommersberger KJ. (2018) Distal radius fractures: Update on imaging. Radiologe. 58(2): 159-174. [PubMed.]
- Harper CM, Dowlatshahi AS, Rozental TD. (2020) Evaluating outcomes following open fractures of the distal radius. J Hand Surg Am. 45(1): 41-47. [PubMed.]
- Kim JY, Moon JW, Ryu BY. (2020) Considerations when diagnosing and treating an extra-articular fracture of distal radius based on plain radiographs. J Hand Surg Asian Pac Vol. 25(4): 489-494. [PubMed.]
- Zhang X, Zhang Y, Fan J, Yuan F, Tang Q, et al. (2019) Analyses of fracture line distribution in intra-articular distal radius fractures. Radiol Med.124(7): 613-619. [PubMed.]
- Wu M, Li X, Li J, Chen Y. (2020) Operative vs conservative treatment in distal radius fractures: a protocol. Medicine (Baltimore). 99(29): e21250. [PubMed.]
- Woolnough T, Axelrod D, Bozzo A, Koziarz A, Koziarz F, et al. (2021) What is the relative effectiveness of the various surgical treatment options for distal radius fractures? A systematic review and network meta-analysis of randomized controlled trials. Clin Orthop Relat Res. 479(2): 348-362. [PubMed.]
- Athar SM, Ashwood N, Aerealis G, Bain GI. (2018) Is external fixation a better way than plaster to supplement K-wires in non-comminuted distal radius fractures? Postgrad Med J. 94(1107): 20-24. [PubMed.]
- Cheng P, Wu F, Chen H, Jiang C, Wang T, et al. (2020) Early hybrid nonbridging external fixation of unstable distal radius fractures in patients aged ≥ 50 years. J Int Med Res. 48(4): 300060519879562. [PubMed.]
- Simic PM, Placzek JD. (2007) Distal radius fracture. In: Stannard JP, Schmidt AH, Kregor PJ. Surgical Treatment of Orthopaedic Trauma. New York: Thieme. p.364-386. [Ref.]
- Ficke B, Ransom EF, Hess MC, Moon AS, McKissack HM, et al. (2018) Outcomes of staged treatment for complex distal radius fractures. Cureus 10(9): e3273. [Ref.]
- Konrads C, Gonser C, Bahrs C. (2021) Fractures of the distal radius. Z Orthop Unfall. 159(2): 217-231. [PubMed.]
- Wu JC, Strickland CD, Chambers JS. (2019) Wrist fractures and osteoporosis. Orthop Clin North Am. 50(2): 211-221. [Ref.]
- Hajianpour MA, Sheikh B, Feanny M, Berkowitz M, Latta LL. (2020) Treatment of selected distal radius fractures with nonbridging external fixation. J Long Term Eff Med Implants. 30(3): 199-204. [PubMed.]
- Aita MA, Rodrigues FL, Alves KHCR, de Oliveira RK, Ruggiero GM, et al. (2019) Bridging versus nonbridging dynamic external fixation of unstable distal radius fractures in the elderly with polytrauma: a randomized study. J Wrist Surg. 8(5): 408-415. [Ref.]
- Dwyer CL, Crosby NE, Cooney T, Seeds W, Lubahn JD. (2017) Treating unstable distal radius fractures with a nonspanning external fixation device: comparison with volar locking plates in historical control group. Am J Orthop (Belle Mead NJ). 46(5): E344-E352. [PubMed.]
- Hanus M, Hanák F, Štastný E, Trc T. (2020) Surgical treatment of fractures of the distal radius - ORIF vs external fixation with ligamentotaxis. Rozhl Chir. 99(8): 343-349. [PubMed.]
- Rosenauer R, Pezzei C, Quadlbauer S, Keuchel T, Jurkowitsch J, et al. (2020) Complications after operatively treated distal radius fractures. Arch Orthop Trauma Surg 140(5): 665-673. [PubMed.]
- Yuan ZZ, Yang Z, Liu Q, Liu YM. (2018) Complications following open reduction and internal fixation versus external fixation in treating unstable distal radius fractures: Grading the evidence through a meta-analysis. Orthop Traumatol Surg. 104(1): 95-103. [PubMed.]
- Yu X, Yu Y, Shao X, Bai Y, Zhou T. (2019) Volar locking plate versus external fixation with optional additional K-wire for treatment of AO type C2/C3 fractures: a retrospective comparative study. J Orthop Surg Res. 14(1): 271. [PubMed.]
- Wang WL, Ilyas AM. (2020) Dorsal bridge plating versus external fixation for distal radius fractures. J Wrist Surg. 9(2): 177-184. [Ref.]
- Shukla R, Jain RK, Sharma NK, Kumar R. (2014) External fixation versus volar locking plate for displaced intra-articular distal radius fractures: a prospective randomized comparative study of the functional outcomes. J Orthop Traumatol. 15(4): 265-270. [PubMed.]
- Lee DJ, Elfar JC. (2014) External fixation versus open reduction with locked volar plating for geriatric distal radius fractures. Geriatr Orthop Surg Rehabil. 5(3): 141-143. [Ref.]
- Curtin CM, Hernandez Boussard T. (2014) Readmissions after treatment of distal radius fracture. J Hand Surg Am. 39(10): P1926-1932. [Ref.]
- Li-hai Z, Ya-nan W, Zhi M, Li-cheng Z, et al. (2015) Volar locking plate versus external fixation for the treatment of unstable distal radial fractures: a meta-analysis of randomized controlled trials. J Surg Res. 193(1): 324-333. [Ref.]
- Bajwa AS, Rammappa M, Lee L, Nanda R. (2015) Treatment of unstable distal radius fracture: non-invasive dynamic external fixator versus volar locking plate-functional and radiological outcome in a prospective case-controlled series. SICOT J. 1: 34. [PubMed.]
- Williksen JH, Husby T, Hellund JC, Kvernmo HD, Rosales C, et al. (2015) External fixation and adjuvant pins versus volar locking plate fixation in unstable distal radius fractures: a randomized, controlled study with a 5-year follow-up. J Hand Surg Am. 40(7): P1333-1340. [Ref.]
- Chilakamary VK, Lakkireddy M, Koppolu KK, Rapur S. (2016) Osteosynthesis in distal radius fractures with conventional bridging external fixator; tips and tricks for getting them right. J Clin Diagn Res. 10(1): RC05-RC08. [Ref.]
- Ma C, Deng Q, Pu H, Cheng X, Kan Y, et al. (2016) External fixation is more suitable for intra-articular fractures of the distal radius in elderly patients. Bone Res. 4: 16017. [Ref.]