>Corresponding Author : Mohd Radzi Hilmi
>Article Type : Research Article
>Volume : 1 | Issue : 1
>Received Date : 16 September, 2021
>Accepted Date : 1 October, 2021
>Published Date : 5 October, 2021
>DOI : https://doi.org/10.54289/JORVC2100102
>Citation : Hilmi MR, Kamal KM, Azemin MZC, Razak ZA, Ithnin MH (2021) Repeatability and Reproducibility of Pterygium Grading Based on Clinical Translucence Appearance. J Ophthalmic Res Vis Care 1(1). doi https://doi.org/10.54289/JORVC2100102
>Copyright : © 2021 Hilmi MR, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Research Article | Open Access | Full Text
1Department of Optometry and Visual Sciences, Kulliyyah of Allied Health Sciences, Inter-national Islamic University Malaysia (IIUM), Kuantan, Pahang, Malaysia
2Department of Ophthalmology, Kulliyyah of Medicine, International Islamic University Malaysia (IIUM), Kuantan, Pahang, Malaysia
*Corresponding author: Mohd Radzi Hilmi, Department of Optometry and Visual Science, Kulliyyah of Allied Health Sciences, IIUM, Jalan Sultan Ahmad Shah, 25200 Bandar Indera Mahkota, Kuantan, Pahang, Malaysia
Abstract
Background: The goal of this study was to evaluate the repeatability and reproducibility of pterygium grading based on clinical translucence appearances and its reliability in clinical setting.
Methods: A total of 93 primary pterygium eyes from 93 participants who visited a tertiary ophthalmic clinic were recruited in this study. Two (2) ophthalmologists and two (2) optometrists evaluated and graded the 93 primary pterygium images in randomized fashion. Graders were instructed to utilise the clinical translucence appearance of pterygium to grade them into type I, II and III. Repeatability testing was done by a single expert by comparing grading of each image on two separate sessions, with one month interval between sessions. Reproducibility was tested by comparing the grading obtained by both experts and optometrists.
Results: Paired and independent T-test results showed no significance difference between graders for both experts and optometrists’ group (all P > 0.05). Intra-grader and inter-grader reliability estimates were high with intraclass correlation ranging from 0.97 to 0.98 for both groups.
Conclusions: Pterygium clinical grading based on its translucence appearance is reliable and repeatable in clinical setting, easily to be graded, interpreted, and recommended for clinicians with different levels of experience.
Keywords: pterygium; translucency; fleshiness; clinical grading; reliability
Abbrivations: UV: Ultraviolet, IIUM: International Islamic University Malaysia, IREC: research ethical committee, SPSS: Predictive analytics software, ICC: intraclass correlation coefficients, LoA: limits of agreement.
Introduction
Pterygium is an abnormal benign lesion which originates from the bulbar conjunctiva and progresses towards the central cornea [1-3]. It is an established fact that prevalence of pterygium is closely related to ultraviolet (UV) ray exposures [4-6]. Pterygium is also known as one of the established factors which contribute to induced corneal astigmatism [7-12]. However, to date, it is difficult to predict its progression due to its non-specific tissue growth in nature.
Clinically, there are several grading’s been employed in assessing pterygium. Pterygium is assessed based on several approaches such as via its morphology [13], extension or length [7,8,14,15], its size [16-21] and based on its encroachment relative to the corneal size [7,8,15,22]. Although these approaches are clinically relevant, the main lacking in these gradings are lack of consistency in measurement as they were subjectively measured. Hence, individual variation is an issue which could lead to subjective bias. In 1997, Donald Tan and his team [13] had proposed a classification of pterygium which is based on its clinical translucence appearance (Figure 1).
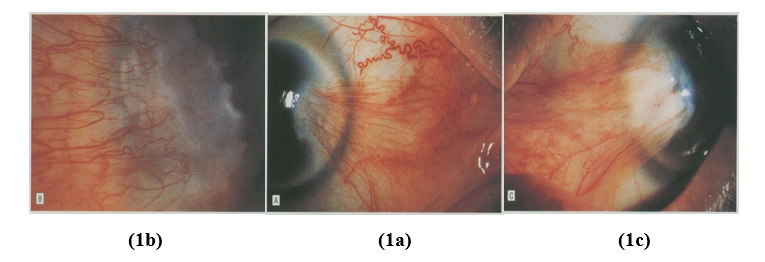
Figure 1: Reference images of Tan’s pterygium clinical grading, (a) Grade I. (b) Grade II. (c) Grade III
They [13] proposed a clinical grading which was based on three (3) types or grades known as atrophy, intermediate and fleshy. The framework of this theory was the loss of translucency of pterygium tissue is related to increased fleshiness that could represent the fibrovascular component of pterygium. The authors [13] divided these classifications into three (3) grades as described below:
- Grade-I (atrophy) - denoted as pterygium which episcleral vessels underlying the body of pterygium were unobscured and clearly distinguished (Figure 1a).
- Grade-II (intermediate) - denoted as pterygium which episcleral vessel details were indistinctly seen or partially obscured (Figure 1b).
- Grade-III (fleshy) - denoted as pterygium which episcleral vessels underlying the body of pterygium were totally obscured (Figure 1c).
To the best of our literature search, no study has been done in proving the repeatability and reliability of Tan’s classification of pterygium. Hence, this study aims to establish the reliability and repeatability of the subjectively measured Tan’s clinical grading of pterygium utilizing two (2) ophthalmologists and two (2) optometrists with different years of experience in the field. This is important to ensure that individual variations in subjective clinical grading are kept minimum.
Methods
93 primary pterygium eyes from 93 patients were recruited in this study. This study applied digitized pterygium images and other data obtained during the baseline visit. Image acquisition, image analyses and its clinical grading were identical as in our previous work [23-26]. A group of 93 primary pterygium patients from 93 individuals who visit an eye-specialist were selected in order to display a wide range of severity of pterygium patients. All participants in this study were selected based on specific criteria as previously described [23-26]. Assessment, diagnosis and classification of primary pterygium were performed by a single ophthalmologist (KMK). The study was conducted according to recommendation of the tenets of the Declaration of Helsinki and approved by the International Islamic University Malaysia (IIUM) research ethical committee (IREC) (IIUM/310/G13/4/4-125). Written and informed consent was obtained from all participants prior to any procedures performed. Image acquisition and description of clinical grading were similar as previously described [23-26].
For repeatability testing, each grader (MRH, KMK, ZAR and MHI) was given two (2) sets of images consisting of 93 pterygium images in each set were randomized using randomization software [27]. Each set of images was tested in two (2) different sessions. The time interval between the first and second session was set at least a month apart. The results between sessions were compared to determine its individual repeatability. For reproducibility testing, each grader (MRH, KMK, ZAR and MHI) graded each of 93 images based on Tan’s classification of pterygium [13]. The set of images for both assessors were also randomized as described above. The redness appearance was graded by both corneal experts (KMK and ZAR) and experienced (MRH) and inexperienced optometrist (MHI) were based on the clinical scales and reference images as in previous work [13]. Figure 1 below showed the illustration of the reference images.
All 93 images were presented using PowerPoint™ presentation (Microsoft Corporation, Redmond, WA, USA) and displayed on a monitor with 17-inch 1280 X 1024 resolution. This is important to ensure the quantification and evaluation processes conform to normal human colour perception. Statistical analyses were performed using IBM SPSS (Predictive analytics software) (Version 19, SPSS Inc., Chicago, IL, USA). Paired T-test was employed to descriptively evaluate the difference between two sessions, while independent T-test was employed to evaluate difference between graders (both experts and between experienced-inexperienced clinicians). The intra-grader repeatability and inter-grader reproducibility were assessed using a combination of intraclass correlation coefficients (ICC) and limits of agreement (LoA) respectively.
Results
The analysis included 93 participants, with 50.5 % (n = 47) were men. The mean and standard deviation (mean ± SD) of pterygium redness based on subjective clinical grading by experts for grader 1 (KMK) was 1.73 ± 0.61 for session 1 (baseline) and 1.70 ± 0.63 for session 2. Paired T-test results showed no significance difference between session 1 and 2 (P = 0.132). For grader 2 (ZAR), the mean ± SD of pterygium redness was 1.72 ± 0.66 for baseline and 1.73 ± 0.53 for session 2 (P = 0.158). Independent T-test results showed no significance difference between both graders (P = 0.596).
With regards to experienced-inexperienced grader 3 (MRH) and 4 (MHI), the mean and standard deviation (mean ± SD) of pterygium redness for grader 3 (MRH) was 1.75 ± 0.65 for baseline and 1.73 ± 0.55 for session 2 (P = 0.193). While for grader 4 (MHI), the mean ± SD of pterygium redness was 1.74 ± 0.66 for baseline and 1.73 ± 0.75 for session 2 (P = 0.216), with independent T-test results showed no significance difference between both graders (P = 0.623). Descriptive results were summarized in Table I below. Normality testing was evaluated using Shapiro-Wilk test, and the results showed normal data distribution.
In comparison between the corneal experts, the intra-observer agreement between initial and second grading 1 month apart was 0.98 (95 % CI, 0.971 - 0.987; P < 0.001). Bland-Altman analysis showed narrow limits of agreement (LoA) of 0.67 which indicates good intra-observer agreement of the redness grading. Inter-observer agreement was 0.97 (95 % CI, 0.964 - 0.984; P < 0.001) with Bland-Altman analysis showing a narrow LoA of 0.76. In comparison between experienced and inexperienced optometrists, the intra-observer agreement between initial and second grading 1 month apart was 0.97 (95 % CI, 0.965 - 0.975; P < 0.001) with Bland-Altman analysis showed narrow limits of agreement (LoA) of 0.72. Inter-observer agreement was found 0.96 (95 % CI, 0.964 - 0.978; P < 0.001) with LoA of 0.75. Table 2 below summarizes the intra and inter-grader reliability estimates based on expert subjective grading and between experienced and inexperienced optometrists which indicates excellent reliability, with ICC of 0.97 to 0.98 and 0.96 to 0.97 respectively.
Discussion
It is an established fact that subjective grading of pterygium is difficult and prone to subjective bias. This is due to the nature of pterygium evaluation itself which requires manual measurement of pterygium based on its horizontal length or its encroachment. However, lack of studies has been done in evaluating pterygium based on its translucency known as Tan’s classification of pterygium. Hence, this study aims to evaluate the agreement of Tan’s classification of pterygium based on a subjectively graded method using two different clinicians with different experiences. It is important as standardization is the key in assessment, diagnosing and monitoring pterygium patients and in any ocular pathology. By having this, the evaluation would be less subjectively biased and less prone to individual variation [28-30]. Hence, error between observers can be minimized and improve its reliability.
The current study results showed that the intra and inter-grader reliability testing in subjectively measured the pterygium redness were excellent with all ICCs were more than 0.90. Bland-Altman analysis revealed narrow LoA for all tests. Narrow LoA of less than 1.0 indicates good agreement between observers [31]. Previous works [32,33] had employed approximately similar techniques in assessing agreement of clinical grading of the anterior eye. The differences were only in the description of the scales and its scales interval which made it more detailed and specific for each condition. Redness grading is important as it may be applied to describe different severity of primary pterygium [23] and also indirectly indicates presence of inflammatory factors which further promotes progression of a disease due to angiogenesis factor from microvessel density perspective [34-38].
There are few ways in assessing repeatability and reliability of a clinical grading such as by employing more images, hence less number of grader and vice versa. Both CCLRU proposed by Terry et al.,[32] and the EFRON clinical grading proposed by Efron [33] employed the latter approach by labouring multiple and vast number of graders in evaluating clinical grading of the corneal complication. The drawback of this approach is it is time-consuming and standardization of time and location setting of the grading was also difficult to be made.
Other previous works [23-26,28,39] employed the less labour-intensive approach by employing more images in a standardized form and clinical setting using visual technology as demonstrated in this study. This approach proved to be better in terms of standardization as all images were presented in a uniform manner with standardization of illumination and brightness. However, it is worth noting that a possible confounding factor for this approach is how normal the colour vision status of the grader is. However, this can be easily solved by assessing the normality of colour vision of each grader as suggested in previous work [40].
Conclusion
Pterygium clinical grading based on its translucence appearance is reliable and repeatable in clinical settings and easily to be graded and interpreted.
Disclosure
The author and authors report no conflicts of interest in this work.
References
- Ang LPK, Chua JLL, Tan DTH. (2007) Current concepts and techniques in pterygium treatment. Curr Opin Ophthalmol 18(4): 308-313. [PubMed.]
- Errais K, Bouden J, Mili-boussen I, Anane R, Beltaif O, et al. (2008) Effect of pterygium surgery on corneal topography. Eur J Ophthalmol 18(2): 177-181. [PubMed.]
- Manzar N, Mahar PS. (2013) Pterygium recurrence related to its size and corneal involvement. J Coll Physicians Surg Pak 23(2): 120-123. [PubMed.]
- Liu L, Wu J, Geng J, Yuan Z, Huang D. (2013) Geographical prevalence and risk factors for pterygium: a systematic review and meta-analysis. BMJ Open 3(11): e003787. [Ref.]
- Marmamula S, Khanna RC, Rao GN. (2013) Population-based assessment of prevalence and risk factors for pterygium in the South Indian state of Andhra Pradesh: the Andhra Pradesh Eye Disease Study. Invest Ophthalmol Vis Sci 54(8): 5359-5366. [PubMed.]
- Maharjan IM, Shreshth E, Gurung B. (2014) Prevalence of and associated risk factors for pterygium in the high-altitude communities of Upper Mustang, Nepal. Nepal J Ophthalmol 6(11): 65-70. [PubMed.]
- Hilmi MR, Musa NH, Khairidzan MK, Azemin MZC, Maruziki NN, et al. (2019) Changes in Apical Corneal Curvature in Unilateral Primary Pterygium and Normal Adults Using Simulated-K and Corneal Irregularity Measurement. Int J Allied Health Sci. 3(2): 588-594. [Ref.]
- Mohammad-Salih PAK, Sharif AFMD. (2008) Analysis of pterygium size and induced corneal astigmatism. Cornea 27(4): 434-438. [PubMed.]
- Kheirkhah A, Safi H, Nazari R, Behrouz MJ, Raju VK, et al. (2012) Effects of pterygium surgery on front and back corneal astigmatism. Can J Ophthalmol 47(5): 423-428. [PubMed.]
- Oltulu R, Demirel S, Sarac O, Ozer MD. (2013) Evaluation of corneal and anterior chamber changes following pterygium surgery using a pentacam scheimpflug system: a prospective study. Semin Ophthalmol 28(4): 206-209. [PubMed.]
- Misra S, Craig JP, McGhee CN, Patel DV. (2014) A prospective Study of Pterygium excision and conjunctival autograft with human fibrin tissue adhesive: Effects on vision, refraction and corneal topography. Asia Pac J Ophthalmol (Phila) 3(4): 202-206. [PubMed.]
- Sarac O, Demirel S, Oltulu R. (2014) Efficacy on intralesional bevacizumab administration in primary pterygium: a quantitative analysis. Eye Contact Lens 40(1): 46-50. [PubMed.]
- Tan DT, Chee SP, Dear KB, Lim AS. (1997) Effect of pterygium morphology on pterygium recurrence in a controlled trial comparing conjunctival autografting with bare sclera excision. Arch Ophthalmol 115(10): 1235-1240. [PubMed.]
- Gumus K, Erkilic K, Topaktas D, Colin J. (2011) Effect of Pterygia on refractive Indices, Corneal Topography, and Ocular Aberrations. Cornea 30(1): 24-29. [PubMed.]
- Farhood QK, Kareem AA (2012) Pterygium and induced astigmatism. Kufa Med J 15(1): 341-345. [Ref.]
- Oner FH, Kaderli B, Durak I, Cingil G. (2000) Analysis of the pterygium size inducing marked refractive astigmatism. Eur J Ophthalmol 10(3): 212-214. [PubMed.]
- Tomidokoro A, Myata K, Sakaguchi Y, Samejima T, Tokunaga T, et al. (2000) Effects of pterygium on corneal spherical power and astigmatism. Ophthalmology 107(8): 1568-1571. [PubMed.]
- Bahar I, Loya N, Weinberger D, Avisar R. (2004) Effect of pterygium surgery on corneal topography: a prospective study. Cornea 23(2): 113-117. [PubMed.]
- Jaffar S, Dukht U, Rizvi F. (2009) Impact of pterygium size on corneal topography. RMJ 34:145-147. [Ref.]
- Altan-Yaycioglu R, Kucukerdonmez C, Karalezli A, Fatma C, Yonca AA. (2013) Astigmatic changes following pterygium removal: comparison of 5 different methods. Indian J Ophthalmol 61(3): 104-108. [Ref.]
- Vives PP, Castanheira AMCM, Mora GJ, et al. (2013) Topographic corneal changes in astigmatism due to pterygium’s limbal-conjunctival autograft surgery. J Emmetropia 4: 13-18. [Ref.]
- Avisar R, Loya N, Yassur Y, Weinberger D. (2000) Pterygium-induced corneal astigmatism. Isr Med Assoc J 2: 14-15. [PubMed.]
- Mohd Radzi H, Mohd Zulfaezal CA, Khairidzan MK, Tamrin MIM, Gaffur NA, et al. (2017) Prediction of changes in visual acuity and contrast sensitivity function by tissue redness after pterygium surgery. Curr Eye Res 42: 852-856. [PubMed.]
- Azemin MZC, Hilmi MR, Kamal MK. (2014) Supervised pterygium fibrovascular redness grading using generalized regression neural network. In Fujita H (Ed). New Trends in Software Methodologies, Tools and Techniques. Amsterdam: IOS Press; 2014: 650-656. [PubMed.]
- Che Azemin MZ, Hilmi MR, Mohd Tamrin MI. et al. (2014) Fibrovascular redness grading using Gaussian process regression with radial basis function kernel. In Biomedical Engineering and Sciences (IECBES). IEEE 2014.113–116. [Ref.]
- Che Azemin MZ, Mohd Tamrin MI, Hilmi MR, Kamal KM. (2015) GLCM texture analysis on different color space for pterygium grading. ARPN J Eng Appl Sci .10:6410-6413. [Ref.]
- Urbaniak GC, Plous S. Research Randomizer. 2013. [Ref.]
- Peterson RC, Wolffsohn JS. (2009) Objective grading of the anterior eye. Optom Vis Sci. 86(3):273-278. [PubMed.]
- Schulze MM, Jones DA, Simpson TL. (2007) The development of validated bulbar redness grading scales. Optom Vis Sci. 84(10):976-983. [PubMed.]
- Schulze MM, Hutchings N, Simpson TL. (2011) Grading bulbar redness using cross-calibrated clinical grading scales. Invest Ophthalmol Vis Sci. 52(8): 5812-5817. [Ref.]
- Bland JM, Altman DG. (2007) Agreement between methods of measurement with multiple observations per individual. J Biopharm Stat 17(4): 571-582. [PubMed.]
- Terry RL, Schnider CM, Holden BA, Cornish R, Grant T, et al. (1993) CCLRU Standards for success of daily and extended wear contact lenses. Optom Vis Sci 70(3): 234-243. [PubMed.]
- Efron N. (1998) Grading scales for contact lens complications. Ophthalmic Physiol Opt 18(2): 182-186. [PubMed.]
- Touhami A, Di Pascuale MA, Kawatika T, Valle MD, Rosa RH, et al. (2005) Characterisation of myofibroblasts in fibrovascular tissues of primary and recurrent pterygia. Br J Ophthalmol 89(3): 269-274. [PubMed.]
- Ribatti D, Nico B, Maxia C, Longo V, Murtas D, et al. (2007) Neovascularization and mast cells with tryptase activity increase simultaneously in human pterygium. J Cell Molec Med 11:585-589. [Ref.]
- Ribatti D, Nico B, Perra MT, Maxia C, Sirigu P, et al. (2009) Correlation between NGF/TrkA and microvascular density in human pterygium. Int J Exp Pathology 90 :615-620. [Ref.]
- Džunic B, Jovanović P, Veselinović D, Petrovic A, Stefanovic I, et al. (2010) Analysis of pathohistological characteristics of pterygium. Bosn J Basic Med Sci 10(4): 307-313. [Ref.]
- Noor Syahira CR, Mohd Radzi H, Khairidzan MK, Muziman MSMM (2020). Association of net pterygium tissue mass (dryweight) in determining changes in oculovisual functions and anterior corneal curvature relative to pterygium types. Int J Allied Health Sci. 4(1): 1042-1048. [Ref.]
- Fieguth P, Simpson T. (2002) Automated measurement of bulbar redness. Invest Ophthalmol Vis Sci 43(2):340-347. [PubMed.]
- Dain SJ. (2004) Clinical color vision tests. Clin Exp Optom 87(4-5): 276-293. [PubMed.]