>Corresponding Author : Andrew S Ryser
>Article Type : Case Report
>Volume : 6 | Issue : 1
>Received Date : 20 April, 2026
>Accepted Date : 04 May, 2026
>Published Date : 08 May, 2026
>DOI : https://doi.org/10.54289/JDOE2600105
>Citation : Ryser AS, Sabol JV, Handel S, Baker G, and Ayer C. (2026) Intraoral Scanning Verse Custom Impression Coping for Implant Crowns. J Dent Oral Epidemiol 6(1): doi https://doi.org/10.54289/JDOE2600105
>Copyright : © 2026 Ryser AS, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Case Report | Open Access | Full Text
1Chief Prosthodontist, MAJ, U.S. Army Advanced Education Program in Comprehensive Dentistry, Fort Bragg, NC, USA
2Program Director, COL, U.S. Army Advanced Education Program in Prosthodontics, US Army, Fort Gordon, GA, USA
3Assistant Program Director, LTC, U.S. Army Advanced Education Program in Prosthodontics, US Army, Fort Gordon, GA, USA
4Assistant Program Director, LTC, U.S. Army Advanced Education Program in Comprehensive Dentistry, Fort Bragg, NC, USA
5Resident, MAJ, U.S. Army Advanced Education Program in Comprehensive Dentistry, Fort Bragg, NC, USA
*Corresponding author: Andrew S Ryser, Chief Prosthodontist, MAJ, U.S. Army Advanced Education Program in Comprehensive Dentistry, Fort Bragg, NC, USA
Abstract
Patients: A 26-year-old male reported to a dental clinic with an implant at the maxillary left central incisor with a provisional restoration. A treatment plan of a ceramic crown on a custom titanium abutment was planned.
Discussion: The soft tissue profile of the peri-implant zone is as significant as the implant restoration itself since soft tissue stability and management around osseointegrated implants are considered focal points for an esthetic success. When an implant is ready to be restored the contours and shape of the healed peri-implant tissue must be accurately recorded or the final restoration may fall short of the desired outcome. This critical information can be recorded via implant level impressions or intra-oral scanning. The accuracy of an impression with a custom impression coping compared to an intra-oral scan after the provisional implant crown has been removed is unknown. This case report demonstrates the differences between a custom impression coping and an intraoral scan for a maxillary central incisor.
Conclusion: This article provides insight into the differences between a PVS impression utilizing a custom impression coping and an intraoral scanner and associated scan body and differences in tissue position. The analysis in this case presentation shows some collapse of the tissue when using the intraoral scanner when compared to a tissue supported PVS impression. More research is needed to critically study the collapse of the peri-implant tissue while utilizing intraoral scanners and development of a technique that would prevent collapse of the peri-implant tissue when using an intraoral scanner
Keywords: Fixed Prosthodontics; Implants; Crowns; Gingiva; Digital
Abbreviations: PFZ: Porcelain-Fused-to-Zirconia
Introduction
Restoration of a dental implant in the esthetic zone can be challenging, yet when surgical placement is planned correctly, the challenge may be lessened [1,2]. Virtual planning may illuminate when it is necessary to correct hard or soft tissue deficiencies, before or after implant placement, to achieve an ideal esthetic result [3]. It can be argued that the soft tissue profile of the peri-implant zone is as significant as the implant restoration itself since soft tissue stability and management around osseointegrated implants are considered focal points for an esthetic success [4,5].
Many factors control peri-implant esthetics to include: the peri implant marginal bone, supracrestal tissue attachment, implant geometry and size, crestal bone height, interproximal distance to adjacent tooth or implant, tooth form and shape, and gingival biotype [4]. When executing the planning and surgical phases of implant placement, the restoring dentist must consider and manage the soft tissue appropriately to achieve the desire results [6]. Provisional restorations for immediately placed implants can aid in preservation of the natural emergence profile and lead to more predictable outcomes in the final restoration [7,8]. Implant provisional restorations mold and contour the soft tissue during healing, allowing for control of the peri-implant soft tissue when designing the final prosthesis [9,10]. The goal of the provisional restoration can be used to establish the ideal emergence profile, guide the growth of interdental papillae, and shape gingival contours, resulting in ideal soft tissue architecture transferrable to the final restoration [11].
When an implant is ready to be restored, not only is the fixture position and timing recorded, but also the contours and shape of the healed peri-implant tissue [12]. These parameters must be accurately recorded or the final restoration may fall short of the desired outcome [13]. This critical information can be recorded via implant level impressions or intra-oral scanning [14-16].
For all the emphasis that is made regarding soft tissue contours approximating a provisional restoration, the replication of the soft tissue is variable. Custom impression copings replicated from the provisional restoration is a widely used modality for recording the ideal tissue contours [17]. However, the time needed and materials used to form the custom impression coping, as well as the associated soft tissue movement, may lead to some unpredictability of the soft tissue impression. The accuracy of an impression with a custom impression coping compared to an intra-oral scan after the provisional implant crown has been removed is unknown. It is unknown how quickly the peri-implant tissue collapses when the provisional crown is removed [8]. This case reports demonstrates the differences between a custom impression coping and an intraoral scan for a maxillary central incisor.
Materials and Methods
A 26-year-old male reported to a dental clinic with an implant at the maxillary left central incisor position. The implant was restored with a provisional restoration during stage two of the implant surgery (Fig. 1). The patient was treatment planned for a custom titanium abutment and a porcelain-fused-to-zirconia (PFZ) abutment-supported implant crown. The patient was determined to have a thick gingival biotype and the tissue contours of the provisional crown were deemed satisfactory. Informed consent for treatment and publication of case was obtained.
A final impression using a custom tray, PVS impression material, and a custom impression coping were used to complete a pickup impression of the maxillary arch. After the impression was removed from the patient’s mouth, an intraoral scan of the implant was obtained using a Primescan (Dentsply Sirona, USA) less than 30 seconds after removal of the provisional restoration (Fig. 2). The implant impression was poured in type 4 stone, and the cast was scanned using Primescan. The scanned stone cast STL was imported as the referenced data and the intraoral scan STL was imported as the measured data into GeoMagic Control X (Oqton Inc, USA) (Figs. 3 and 4). Initial alignment and then best fit matching of the data STLs were performed in GeoMagic (Fig. 5). The peri- implant tissue (emergence profile and gingival contours) was isolated using the GeoMagic circle tool and the area of interest was examined using the 3D comparison tool (Figs. 6 and 7). The mean value, maximum, and minimum deviations of the gap distance from the reference data points to the measured data points were measured (Table 1).

Figure 1: Intraoral photograph of #9 implant provisional restoration
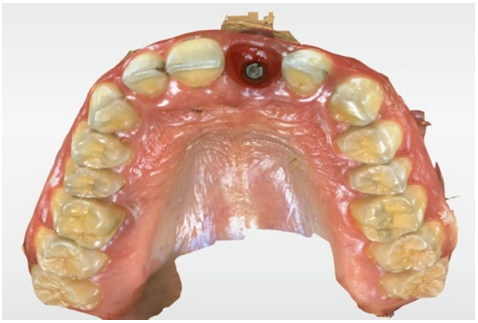
Figure 2: Intraoral scan of #9 implant tissue contours.
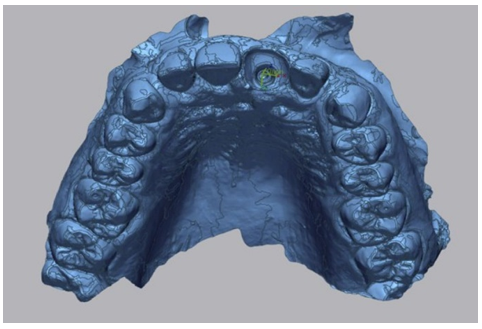
Figure 3: Stone cast STL imported into GeoMagic as reference data.
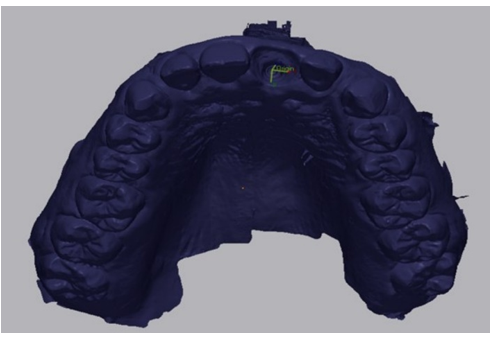
Figure 4: Intraoral scan STL imported into GeoMagic as measurement data.
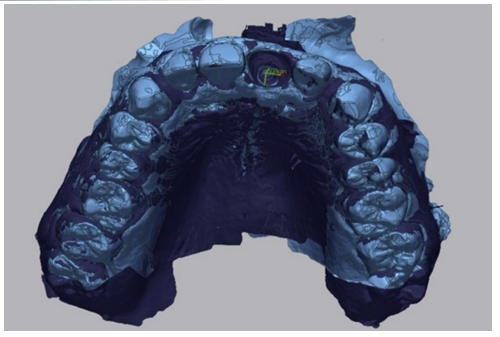
Figure 5: Best match alignment in GeoMagic.
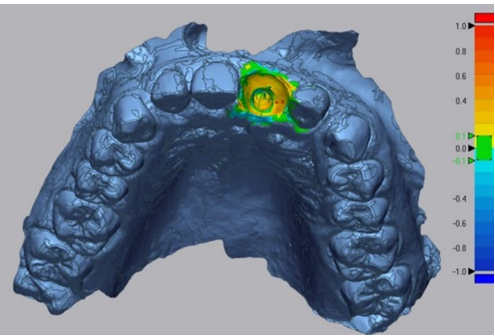
Figure 6: 3D compare analysis of selected data.
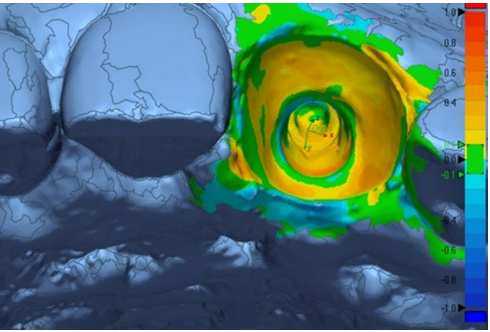
Figure 7: 3D compare analysis of selected data.

Table 1: Minimum, Maximum, and Average Deviation (mm).
Discussion
Provisional restorations play a significant role in tissue contouring and shaping to provide ideal contours for a predictable implant retained restoration [18]. Providers use provisional restorations as a prototype to condition and evaluate critical soft tissue areas such as interdental papillae, gingival contours, and facial support [19]. Accurately capturing the soft tissue contours once the provisional restoration is removed is vital for replicating the soft tissue in the dental laboratory to achieve the most predictable outcome [20]. Hinds described a technique to fabricate a custom impression coping to accurately capture the soft tissue once an implant supported provisional is removed [20]. The custom impression coping prevents the collapse of the soft tissue and is transferred to the cast once poured in stone. This exact replica of the soft tissue allows the dental technician to replicate the desired contours and emergence profile the clinician achieved in the provisional restoration [20].
Intraoral scanning is rapidly replacing conventional impression techniques. This transition to digital technology cannot fully replace traditional methods without further advancement [21]. At this time, very little literature exists that examines the potential collapse of soft tissue when scanning an implant after removal of the provisional restoration. Less research exists comparing intraoral scanning to traditional impression techniques. Intraoral scanners have the capability to easily scan the soft tissue contours after removing the provisional restoration. However, the accuracy of capturing the soft tissue profile through digital scans as compared to the Hinds technique and the custom impression coping is unknown.
This case report demonstrates the differences seen between a PVS impression utilizing a custom impression coping and an intraoral scan by comparing the two in GeoMagic Control X.
The results of the 3D comparison between the PVS impression and intraoral scan indicate that there are deviations between the two techniques in capturing the soft tissue contours of the provisional implant restoration. The average deviation between the two techniques was 0.0391 mm. The maximum deviation from the stone model to the intraoral scan was 0.5291 mm. The 3D comparison color diagram demonstrates that the peri implant tissue in the intraoral scan resulted in some collapse from its original position when compared to the PVS impression that utilized a custom impression coping. The significance of these differences may be amplified with a patient who exhibits a thin biotype or if the lag time between removal of a provisional and the scan is greater than 30 seconds. Despite the perceived efficiency of intraoral scanning, future studies should examine the extent of tissue collapse over time, and whether the custom impression coping can truly be discarded in favor of an unsupported scan.
Summary
This article provides insight into the differences between a PVS impression utilizing a custom impression coping and an intraoral scanner and associated scan body and differences in tissue position. The analysis in this case presentation shows some collapse of the tissue when using the intraoral scanner when compared to a tissue supported PVS impression. There are many factors that affect the potential for tissue to collapse to include tissue biotype, time from provisional crown removal to scan, and tissue health. More research is needed to critically study the collapse of the peri-implant tissue while utilizing intraoral scanners and development of a technique that would prevent collapse of the peri-implant tissue when using an intraoral scanner.
Conflicts of Interest Statement: The authors declare no conflicts of interest regarding this manuscript.
References
- Testori T., Weinstein T., Scutella F., Wang HL., Zucchelli G. Implant placement in the esthetic area: criteria for positioning single and multiple implants. Periodontology 2000. 2018;77:176–96. [PubMed.]
- El Chaar E., White C., Salama T., Andrawis A. Quantifying the Emergence Profile Contour for Immediate Provisionalization: A Proposed Mathematical Model. J Oral Implantol. 2021;47:191–198. [PubMed.]
- Tan WL., Wong TL., Wong MC., Lang NP. A systematic review of post-extractional alveolar hard and soft tissue dimensional changes in humans. Clin Oral Implants Res. 2012;5:1–21. [PubMed.]
- Dhir S. The peri–implant esthetics: An unforgettable entity. J Indian Soc Periodontol. 2011;15:98–103. [PubMed.]
- Giannobile WV., Jung RE., Schwarz F. Evidence-based knowledge on the aesthetics and maintenance of peri-implant soft tissues: Osteology Foundation Consensus Report Part 1–Effects of soft tissue augmentation procedures on the maintenance of peri-implant soft tissue health. Clinical Oral Implants Research. 2018;29:7–10. [PubMed.]
- Hamilton A., Putra A., Nakapaksin P., Kamolroongwarakul P., et al. Implant prosthodontic design as a predisposing or precipitating factor for peri‐implant disease: A review. Clin Implant Dent Relat Res. 2023;25:710–22. [PubMed] [PubMed.]
- Kan JY., Rungcharassaeng K., Lozada J. Immediate placement and provisionalization of maxillary anterior single implants: 1-year prospective study. Int J Oral Maxillofac Implants. 2003;18:31–9. [PubMed.]
- Alshiddi IF., Dent DC. Accurate registration of peri-implant soft tissues to create an optimal emergence profile. Contemp Clin Dent. 2015;6:S122–5. [PubMed.]
- Ganddini MR., Tallents RH., Ercoli C., Ganddini R. Technique for fabricating a cement-retained single-unit implant-supported provisional restoration in the esthetic zone. J Prosthet Dent. 2005;94:296–8. [PubMed.]
- Moscovitch MS., Saba S. The use of a provisional restoration in implant dentistry: A clinical report. Int J Oral Maxillofac Implants. 1996;11:395–9. [PubMed.]
- Iannello G., Fiorillo L., D’Amico C., Minervini G., Terranova A., Cervino G. Presenting a Protocol for Dental Implant Restorations. Prosthesis. 2023;5(4):1153–1170. [Ref.]
- Ender A., Attin T., Mehl A. In vivo precision of conventional and digital methods of obtaining complete-arch dental impressions. J Prosthet Dent. 2016;115:313–20. [PubMed.]
- Tsai BY. A Method for Obtaining Peri-Implant Soft-Tissue Contours by Using Screw-Retained Provisional Restorations as Impression Copings: A Clinical Report. J Oral Implantol. 2011;37:605–9. [PubMed.]
- Chee W., Jivraj S. Impression techniques for implant dentistry. Br Dent J. 2006;201:429–432. [PubMed.]
- Gehrke P., Rashidpour M., Sader R., et al. A systematic review of factors impacting intraoral scanning accuracy in implant dentistry with emphasis on scan bodies. Int J Implant Dent. 2024;10:20. [PubMed.]
- Abduo J., Palamara JE. Accuracy of digital impressions versus conventional impressions for 2 implants: An in vitro study evaluating the effect of implant angulation. Int J Implant Dent. 2021;7(1):75. [PubMed.]
- Ryser AS., Handel S., Sabol JV., Meister D and McLaughlin J. Staged Extractions and Implant Placement for Maxillary Central Incisors: A Case Report. J Dent Oral Epidemiol. 2024;4(1):1-6. [Ref.]
- Tsai BY. Use of provisional restorations as implant impression copings. J Prosthet Dent. 2007;97:395–6. [PubMed.]
- Ferencz JL. Maintaining and enhancing gingival architecture in fixed prosthodontics. J Prosthet Dent. 1991;65:650–7. [PubMed.]
- Hinds KF. Custom impression coping for an exact registration of the healed tissue in the esthetic implant restoration. Int J Periodontics Restorative Dent. 1997;17. [PubMed.]
- Khurshid Z. Digital Dentistry: Transformation of Oral Health and Dental Education with Technology. Eur J Dent. 2023;17(4):943–944. [PubMed.]