>Corresponding Author : Andrew S Ryser
>Article Type : Case Report
>Volume : 5 | Issue : 2
>Received Date : 01 October, 2025
>Accepted Date : 13 October, 2025
>Published Date : 17 October, 2025
>DOI : https://doi.org/10.54289/JDOE2500109
>Citation : Ryser AS, Lopez RM, and Handel S. (2025) Adding a Tooth to a Metal Framework Obturator using CAD/CAM Technology. J Dent Oral Epidemiol 5(2): doi https://doi.org/10.54289/JDOE2500109
>Copyright : © 2025 Ryser AS, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Case Report | Open Access | Full Text
1Chief Prosthodontist, MAJ, U.S. Army Advanced Education Program in Comprehensive Dentistry, Fort Bragg, NC, USA
2Director of CAD/CAM, 59th Dental Support Squadron, Air Force Post Graduate Dental School, Lackland Air Force Base, San Antonio, Texas, USA
3Assistant Program Director, LTC, U.S. Army Advanced Education Program in Prosthodontics, Associate Professor, Post Graduate Dental School, Uniformed Services University, Fort Eisenhower, GA, USA
*Corresponding author: Andrew S Ryser, Chief Prosthodontist, MAJ, U.S. Army Advanced Education Program in Comprehensive Dentistry, Fort Bragg, NC, USA
Abstract
The ramifications of tooth loss after obturator fabrication can present a challenging situation in which there are limited viable solutions. This challenge is only amplified by poor masticatory ability, a change in phonetics, and esthetic concerns that can negatively affect a patient’s psychological and social wellbeing. Replacement of a missing tooth can be accomplished through fixed, repairing or refabricating the removable obturator prosthesis. Although fixed options tend to be the choice of treatment, removable prosthetics can often be the treatment of choice when the edentulous area is too long, surgery is not an option for implants, or a patient’s finances or desires necessitate an alternative to fixed prosthodontics. This article introduces a novel technique to add a tooth to a metal framework obturator utilizing CAD/CAM technology.
A patient presented to a prosthodontic practice with a maxillary obturator and a missing maxillary central incisor. The obturator was well-fitting, and the patient was highly satisfied with the obturator but wanted to replace his missing maxillary central incisor which was lost due to loss of periodontal support. An abutment was designed and cast in ticonium; it was then soldered to the metal framework. A lithium disilicate ceramic crown was milled and cemented to the abutment to replace the missing tooth.
Keywords: Digital Dentistry, CAD/CAM, Removable, Obturator
Abbreviations: FDP: Fixed Dental Prostheses, EOS: Extraoral Scanner, RDP: Removable Partial Dentures
Introduction
Maxillary defects resulting from resection due to cancer, trauma induced reconstruction, or developmental anomalies play an enormous impact on a patient’s function, esthetics, and psychosocial health. Maxillofacial prosthodontists recognize the complexity of treating patients with these debilitating defects, especially when the goal is to restore the patient to their pre-resected form.
The process of fabricating an obturator includes an initial impression of the maxilla and defect which will be used for the construction of a custom tray. The custom tray is used to make a final impression which will be used for the fabrication of the definitive obturator. Even after the delivery of the obturator numerous adjustments can be required for perfecting the fit and increasing the patient’s comfort and functional occlusion. Once adjustments are completed and the patient is satisfied, the loss of a tooth can be devastating.
According to the glossary of prosthodontic term partial edentulism is defined as: a dental condition where a person has lost one or more teeth, but not all of them [1]. The loss of a tooth generally occurs due to several factors to include caries, periodontal disease, trauma, and neoplastic cystic lesions [2,3]. The main reason for tooth loss continues to be untreated caries, while periodontal disease is the second leading cause of tooth loss [3-5]. Although the rate of tooth loss is decreasing, the overall number of patients who are partially dentate is increasing due to an increase in life expectancy and a rise in the number of elderly patients [6]. Campell et al. estimated that the number of partially dentate in the United Stated could rise to over 200 million by 2030 [6]. Patients with maxillary defects are not exempt from tooth loss and are in fact more likely to lose teeth at an accelerated rate especially those with a history of radiation therapy [7].
Patients often require replacement of missing teeth to improve mastication, esthetics, and phonetics, and to prevent drifting or supra-eruption of remaining teeth [6]. Treatment options to replace missing teeth can be divided into two categories: fixed dental prostheses (FDPs) and removable dental prostheses (obturators). Both fixed and removable prostheses can be tooth borne or implant supported. Fixed and removable prostheses offer their own distinct advantages and disadvantages. However, removable prostheses are generally considered a less expensive option, facilitate easier hygiene, and overcome the surgical and biomechanical issues of dental implants [6]. In the case of the patient’s with maxillary defects the etiology will influence the treatment plan and obturators are often the first line of treatment when replacing lost hard and soft tissue, long edentulous spans, improving masticatory function, stabilizing occlusal relationships, and providing support for orofacial structures to improve esthetics [8-10]. Removable partials dentures and obturators can be fabricated 3 different ways: a metal framework, flexible partial, or an acrylic based [10]. Obturators include clasps made of out cobalt chromium, titanium, or plastic to increase stability and retention of the partial [10].
Removable denture prostheses offer patients a reliable treatment option to replace missing teeth when fixed prosthodontics are not an option due to abutment teeth condition, the length of the edentulous space, loss of hard and soft tissues, finances, medical concerns that make surgery unfavorable, or for obturators when surgical closure of the defect is not possible. Once an obturator is delivered patient satisfaction of the obturator can be negatively affected if additional teeth are lost. If an abutment tooth is lost, the obturator usually needs to be redesigned and remade, if a non-abutment tooth is lost it can be challenging to replace the missing tooth. This situation can require that the obturator needs to be remade if the patient wants to replace the lost tooth. This technique article describes a way to replace a tooth on an obturator metal framework by creating a custom abutment that is soldered onto the obturator framework, then a ceramic crown is milled and cemented to the abutment.
Materials and Methods
Case A 56-year-old male presented to a prosthodontic practice with an existing maxillary cast metal framework obturator. The current prosthesis restored the patient’s left maxillary posterior teeth and obturated the resected section of the patient’s palate which was lost due to oral cancer 15 years prior. The patient recently underwent removal of a single maxillary incisor (#9) due to loss of periodontal support and mobility. The existing obturator was well designed and provided the necessary retention, stability and support required for restoring the missing posterior segment, yet the missing tooth was not replaced (Fig. 1). The patient wanted to replace his missing maxillary central incisor; however, he did not want to replace his obturator which was only a year old.

Figure 1: Pre- treatment frontal MIP with obturator.
Due to the reflective properties of the metal base obturator, an alginate impression was made of the obturator in the patient’s mouth. After the impression set, the impression and the patient’s obturator were removed and poured in type IV dental stone while still combined After a retentive groove, palatal to site #9, was created in the RPD framework, the existing obturator and fabricated cast were coated with scanning spray (Scanspray, Renfert, USA) and scanned using an extraoral scanner (EOS) (inEos X5, Dentsply Sirona, USA). Digital scan of the opposing arch, and a buccal bite registration were also obtained using the same EOS. A custom abutment was designed in CAD software (Exocad), milled from wax, and cast in ticonium. Once the abutment was divested, it was seated into the retentive groove created in the framework and laser welded into place using an AlphaLaser ALP50 (Figs. 2 and 3).
Once the ticonium abutment was welded to the framework, the framework and opposing arch were again scanned. A lithium disilicate crown (e.max, Lithium Disilicate, Ivoclar Vivadent, Liechtenstein) was designed and milled using CAD/CAM technology (Primescan and Primemill, Dentsply Sirona, USA). The crown was crystallized, polished, stained and glazed using MIYO (Jensen, USA). The crown was then cemented to the obturator abutment using a resin cement (Multilink Hybrid Abutment cement, Ivoclar Vivadent, Liechtenstein) (Fig. 4). The obturator was delivered to the patient, and the patient left happy to have the missing tooth replaced without having to endure the process of refabricating the obturator (Figs. 5 and 6).
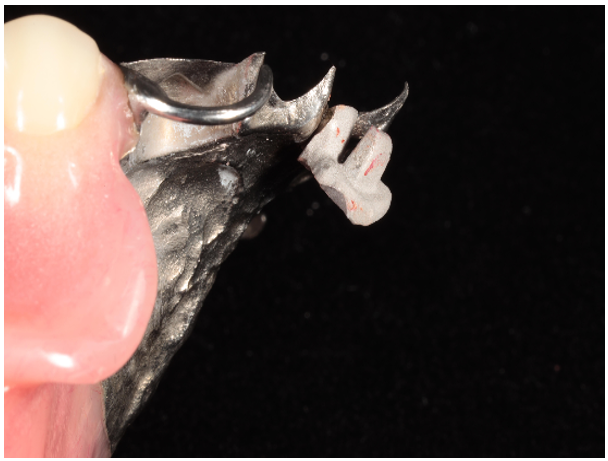
Figure 2: Soldered abutment on obturator framework.
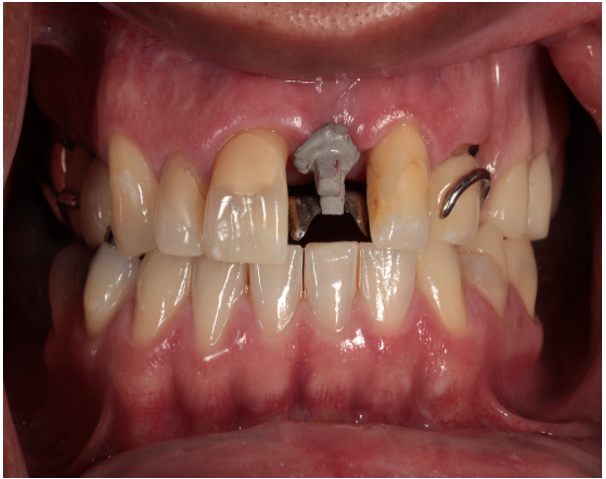
Figure 3: Soldered maxillary central incisor abutment on obturator in the mouth.

Figure 4: Crown being placed on obturator abutment to replace missing maxillary central incisor.

Figure 5: Added maxillary central incisor to maxillary obturator frontal MIP.
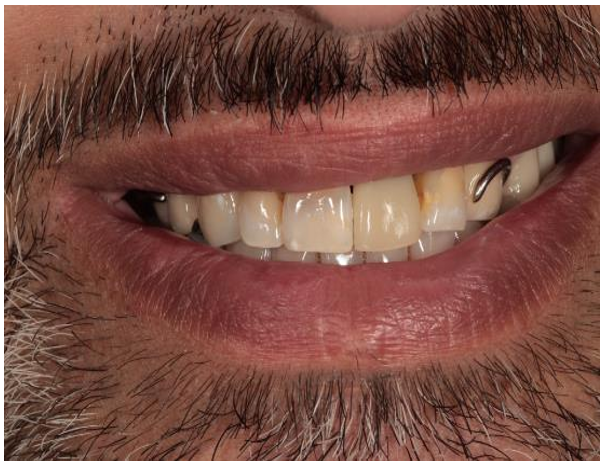
Figure 6: Frontal smile photograph of patient with maxillary obturator and new maxillary central incisor added to obturator.
Discussion
Tooth loss is a major health problem facing a significant portion of the population resulting in not only esthetic and functional concerns, but a decrease in the overall quality of life [11]. Prosthodontics can help replace missing teeth through fixed or removable prosthetics, which increase esthetics, enhances mastication and speech, and improves the psychological and social well-being of patients. Fixed prosthodontics are often the preferred treatment option for patients; however, every partially dentate patient is not a candidate for fixed prosthodontics especially in maxillofacial prosthodontics. Often removable prosthodontics is the treatment of choice when edentulous spans are too long, hard and soft tissue have been lost, surgery isn’t an option due to financial or medical concerns, or when facial structures need support that fixed prosthodontics isn’t able to provide [10].
Removable partial dentures (RDPs) tend to have good satisfaction rates with reports suggesting satisfaction rates between 50-81% [10]. The patient’s satisfaction of their experience with RDPS tends to be based off of several factors to include: patient attitude prior to RDP treatment, gender, age, past experience with removable prosthetics, education provided by the dentist, and fabrication design of the partial denture [12-14]. When looking at the RDP itself the following factors play a significant role in the overall satisfaction of the prosthesis: number of missing teeth and Kennedy classification, arch where prosthesis is replacing teeth, type of obturator RDP (acrylic vs metal-based vs flexible), attachments, and number of clasps [10,15-17].
Patients who are satisfied with their removable prosthesis tend to have positive effects from the replacement of their missing teeth. Socially and psychologically the prosthesis replaces what was lost and allows the patient to smile and talk without the fear of being embarrassed from lost teeth [18]. Asides from the psychological and social benefits of removable prostheses mastication is improved which improves dietary intake and overall nutritional and health status [19]. Once a patient has a prosthesis that fits well, is comfortable, improves mastication, speech, and esthetics it can be challenging for the patient to let go of the prosthesis and start new. Finances might affect the ability of the patient to get a new prosthesis especially in a short period.
This article demonstrates a technique that allows a dentist to add a tooth to a metal framework obturator when a tooth must be extracted, allowing the patient to keep the prosthesis they are satisfied with and lowering the financial burden when additional teeth are lost. This technique is for a well-fitting, well adapted prosthesis with good retention and stability. If the prosthesis has poor stability and retention and/or is ill fitting or is damaged anyway that requires it to be remade this technique should not be used to add a tooth. When the partial is no longer clinically acceptable, the partial denture or obturator should be remade and the reasons for doing so should be explained to the patient carefully. This technique also will not replace the loss of an abutment tooth that was used for clasping. Careful examination of the prosthesis and intraoral tissue to ensure a clinical acceptable prosthesis is required before proceeding with a technique as described in this article.
Summary
This case report provides a novel technique that aims to lengthen the lifespan of a well-fitting obturator or RDP where a patient lost a tooth and would like it to be replaced by an existing prosthesis. The technique uses CAD/CAM technology to design an abutment that is soldered to the metal obturator framework, a crown is the milled and cemented to the abutment. This allows the patient to retain a prosthesis they are satisfied with, while also fixing an esthetic or functional concern caused by loss of tooth.
Acknowledgements
This research did not receive any specific grant from funding agencies in the public, commercial, or non-profit sectors. The authors report no conflicts of interest.
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. The authors report no conflicts of interest.
References
- The Glossary of Prosthodontic Terms 2023. J Prosthet Dent. 2023;1(130):e7–126. [PubMed.]
- Muneeb A. Causes and pattern of partial edentulism/ exodontia and its association with age and gender: semi-rural population, Baqai Dental college, Karachi, Pakistan. IDJSR. 2013;1:13–18. [Ref.]
- Abdel-Rahman HK., Tahir CD., Saleh MM., et al. Incidence of Partial edentulism and its relationship with age and gender. Zanco J Med Sci. 2013;17:463–70. [Ref.]
- Zaigham Mueed A., Muneer MU. Pattern of partial edentulism and its association with age and gender. Pakistan Oral and Dental Journal. 2010;30(1):260–63. [Ref.]
- Al-Shammari KF., Al-Ansari JM., Al-Melh MA., Al-Khabbaz AK. Reasons for tooth extraction in Kuwait. Med. Princ. Pract. 2006;15:417–422. [PubMed.]
- Campbell SD., Cooper L., Craddock H., Hyde TP., Nattress B., Pavitt SH., et al. Removable partial dentures: The clinical need for innovation. J Prosthet Dent. 2017;118:273-280. [PubMed.]
- Brennan MT., Treister NS., Sollecito TP., Schmidt BL., Patton LL., Lin A., et al. Tooth Failure Post-Radiotherapy in Head and Neck Cancer: Primary Report of the Clinical Registry of Dental Outcomes in Head and Neck Cancer Patients (OraRad) Study. International Journal of Radiation Oncology*Biology*Physics. 2022;113:320–30. [PubMed.]
- Benso B., Kovalik AC., Jorge JH., & Campanha NH. Failures in the rehabilitation treatment with removable partial dentures. Acta Odontologica Scandinavica. 2013;71(6):1351–1355. [PubMed.]
- Bohnenkamp DM. Removable partial dentures: clinical concepts. Dental Clinics. 2014;58(1):69-89. [PubMed.]
- Awawdeh M., Alotaibi MB., Alharbi AH., Alnafisah SA., Alasiri TS., Alrashidi NI. A Systematic Review of Patient Satisfaction with Removable Partial Dentures (OBTURATORs). Cureus. 2024;7:16(1):e51793. [PubMed.]
- Alshehri MD., Alqahtani WM., Asiri EM., Asiri MN. Awareness to consequences of teeth missing and prosthodontics treatment options among people of Aseer region., Saudi Arabia. J Family Med Prim Care. 2021;10:307-311. [PubMed.]
- Frank RP., Brudvik JS., Leroux B., et al. Relationship between the standards of removable partial denture construction, clinical acceptability, and patient satisfaction. J Prosthet Dent. 2000;83:521–527. [PubMed.]
- Chen J., Ahmad R., Suenaga H., Li W., Sasaki K., Swain M., et al. Shape Optimization for Additive Manufacturing of Removable Partial Dentures--A New Paradigm for Prosthetic CAD/CAM. PLoS One. 2015;10:e0132552. [PubMed.]
- Frank RP., Brudvik JS., Leroux B., Milgrom P., Hawkins N. Relationship between the standards of removable partial denture construction., clinical acceptability., and patient satisfaction. J Prosthet Dent. 2000;83:521-7. [PubMed.]
- Knezović Zlatarić D., Celebić A., Valentić-Peruzović M., Jerolimov V., Pandurić J. A survey of treatment outcomes with removable partial dentures. J Oral Rehabil. 2003;30:847-54. [PubMed.]
- Fueki K., Yoshida-Kohno E., Inamochi Y., Wakabayashi N. Patient satisfaction and preference with thermoplastic resin removable partial dentures: a randomised cross-over trial. J Prosthodont Res. 2020;64:20-25. [PubMed.]
- Hartog L., Meijer HJ., Santing HJ., Vissink A., Raghoebar GM. Patient satisfaction with single-tooth implant therapy in the esthetic zone. Int J Prosthodont. 2014;27:226-8. [PubMed.]
- Nono D., Bagenda G., Okullo I., Rwenyonyi CM. Exploring lived experiences on the usage of removable complete dentures among edentulous patients attending Makerere University Dental Hospital., Kampala., Uganda. BMC Oral Health. 2024;24:709. [PubMed.]
- Moynihan P., Varghese R. Impact of Wearing Dentures on Dietary Intake., Nutritional Status., and Eating: A Systematic Review. JDR Clin Trans Res. 2022;7:334-351. [PubMed.]