>Corresponding Author : Getaneh Haile Minda
>Article Type : Research Article
>Volume : 5 | Issue : 1
>Received Date : 02 March, 2025
>Accepted Date : 14 March, 2025
>Published Date : 1 April, 2025
>DOI : https://doi.org/10.54289/JDOE2500101
>Citation : Minda GH, Kebie A, Tola HH and Amahare AF. (2025) Magnitude of Oral Hygiene Practice its Associated Factor among Elementary School Students in Fiche Town, Oromia, Ethiopia. J Dent Oral Epidemiol 5(1): doi https://doi.org/10.54289/JDOE2500101
>Copyright : © 2025 Minda GH, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Research Article | Open Access | Full Text
Department of public health, College of medicine health science, Salale University, Fiche, Ethiopia
*Corresponding author: Getaneh Haile Minda, Department of public health, College of medicine health science, Salale University, Fiche, Ethiopia
Abstract
Background: Neglected elementary school students were susceptible to dental caries, gingivitis, periodontitis, tooth loss, halitosis, fungus infections, and various gum disorders. Additionally, poor oral hygiene practice has a negative impact on social relationships and behavior; there is limited information on how primary school students practice oral hygiene. This study aimed to determine oral hygiene practice and its associated factors among elementary school students in Fiche Town, Oromia, Ethiopia, in 2022.
Methods: A cross-sectional study design was conducted from April 29 to May 29 in Fiche towns, Oromia, Ethiopia, among elementary school students. A multi-stage probability sampling technique was used to select individuals, classes, and schools. The total sample size was 534 elementary school students. A structured questionnaire was used to collect the data. Data was entered into epi-data version 4.6 and analyzed with SPSS version 26.0. Variables that scored a pvalue of less than 0.2 during the bivariate analysis were included in multilevel logistic regression. The odd ratio with a 95% confidence interval was estimated at the level of significance set at 0.05.
Result: The magnitude of good oral hygiene practices among students was 295 (55.2%). About 284 (53.2%) of students brush their teeth, while 147 (27.5%) do it twice per day and 40 (7.5%) three times or more. More than one-third (449, or 84.1%) have good knowledge. Being female, the student’s mother, whose occupation was a homemaker, and school personal hygiene inspection were significantly associated with good oral hygiene practice among elementary school students.
Conclusion: Overall, good OHP among elementary school students in Fiche Town was very low. Home caretakers of children and hygiene inspections in school were important to enhance elementary school student’s oral hygiene practices.
Keywords: Oral Hygiene Practice, Health-Related Clubs, School Hygiene Inspection, Elementary School, Fiche Town
Abbreviations: AOR: Adjusted Odd Ratio, CI: Confidence Interval, COR: Crude Odd Ratio, DC: Dental Care, DHS: Demographic Health Survey, NCD: Non-Communicable Disease, OHP: Oral hygiene Practice
Introduction
Oral health is the absence of conditions that affect a person’s ability to bite, chew, smile, talk, and maintain their Psychosocial well-being, such as mouth and face discomfort, oral and throat cancer, oral infections and ulcers, periodontal (gum) disease, tooth decay, and tooth loss [1–4]. Oral hygiene practice is for an individual to clean supra gingival plaque [4]. Oral health may have an influence on a person’s appearance, social relationships, and routine physical and mental tasks [4], [5]. A significant aspect of oral health is periodontal health, which focuses on preventing inflammatory illnesses in the connective tissue supporting the teeth [4]. Multiple factors, including lifestyle modifications, restricted access to dental treatment, socioeconomic level, education, and personality, might have an impact on oral health. By maintaining good oral hygiene practices, such as cleaning teeth, using dental floss, quitting smoking, and scheduling routine dentist appointments, oral illnesses can be prevented [3,5]. Dental caries and periodontal disease can be avoided by practicing good oral hygiene, which includes brushing teeth two times per day, using dental floss, and having regular dental examinations [6]. When you brush your teeth, whether with a manual or powered toothbrush, plaque is removed from the teeth and gums, and the biofilm that the plaque bacteria reside in is damaged [7].
Oral diseases are a big public health problem all around the world. The prevalence of oral diseases has increased, mainly for individuals from low socio-economic groups [8]. Poor oral conditions affect 3.9 billion people worldwide; the WHO added oral health to the list of prioritized non-communicable diseases (NCDs) due to this high prevalence rate, particularly given that it shares risk factors with other NCDs like diabetes, cardiovascular disease, and Cancer. Poverty increases the vulnerability of individuals to dental caries; this means that about 80% of people living in sub-Saharan Africa are at increased risk [1]. Poor oral hygiene can result in dental caries, gingivitis, periodontitis, tooth loss, bad breath (halitosis), fungal infections, and various gum diseases. The use of a toothbrush is the most important measure for oral hygiene [2]. Dental caries is an infectious microbial disease of the teeth, and the World Health Organization (WHO) found it to be one of the most prevalent diseases across the world in 2017 [9].
Despite considerable evidence on oral hygiene practice, there was still not studying in developing countries, including Ethiopia. Moreover, although there is an oral hygiene problem in elementary school, there is limited evidence regarding an oral hygiene practice and school supervision of oral hygiene among elementary school students. In addition, there is no information on the factors that affect elementary schools not to practice good oral hygiene. Therefore, this study aims to determine the magnitude of oral hygiene practice and associated factors among elementary school students.
Methods
Study area/setting and period
We conducted the study on Fiche Town elementary school students from March 15 to April 15, 2022. Based on population estimation in 2021/2022 by the Central Statistical Agency of Ethiopia in 2007, the total population of the town is 51041. There are 13 primary schools, of which eight are for 5–8 grade students and five are for 1-4 grade students. Based on the data obtained from the education bureau, a total of 9292 primary school students are currently enrolled in education.
Study design
The institution-based cross-sectional study design was used to assess oral hygiene practice among primary school students.
Population Inclusion and exclusion criteria
All grade 5–8 students of the academic year 2021/22 in eight primary schools in the Fiche town were included in this study. Mentally and physically incapable students were excluded from this study.
Sample size determination
The sample size was calculated using a single population proportion formula by assuming a 70% true population prevalence of poor personal hygiene among the students [10], a 5% margin of error, a 95% confidence interval, and a 1.5 design effect. After calculating the sample size was 323; to account for the design effect, the sample size is multiplied by 1.5, and the total sample size becomes 1.5 * 323 = 485. The sample size further increased by 10% for contingency, which related to non-response, and the total sample size was 534 students.
Sampling Procedure
A multi-stage probability sampling procedure with three stages; the first stage was schools; the second was classes and the third, individual students, was used to select participants from each grade at schools. Of the thirteen primary schools and eight schools that teach students in grades 5–8 found in the town, more than 50% were selected with the simple random sampling method. Of the total 4818 students who were enrolled in grades 5–8 in the 2021/22 academic year, 534 students were selected by proportion to the total number of students in school, and each student was selected by the simple random sampling method using a list of students’ names in each section as a sample frame (Fig 1).
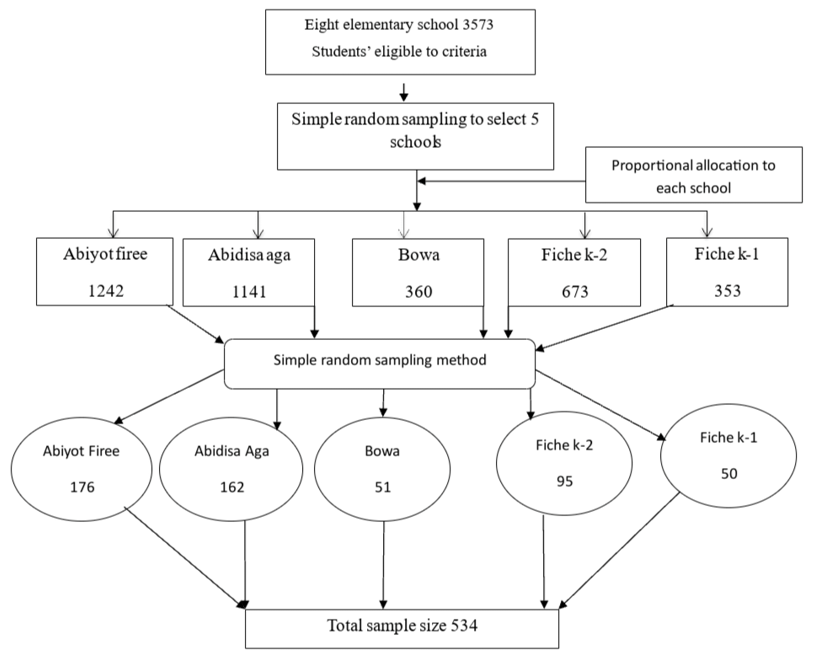
Figure 1: Schematic representation of the sampling procedure Fiche town, Oromia, Ethiopia, 2022.
Data Analysis
The collected data was cleaned and coded by running frequencies and data exploration methods. The data was exported to SPSS (Statistical Package for the Social Sciences) version 26 for the analysis of descriptive statistics such as frequency and percentage for categorical variables and the mean, median, and standard deviations for continuous variables computed. The data was presented with text, tables, and graphs. Multilevel logistic regression models are used to assess the factors associated with good oral hygiene practice.
The first level was each school; the second level was classes; and the third level was individual students’ levels of behaviour. Variables scoring a p-value less than or equal to 0.2 during bivariate analysis were included in the multivariable model to assess the independent effect of each risk factor. The multicollinearity of independent variables was checked by a variance inflation factor (VIF). The adjusted odds ratio with 95% confidence intervals was estimated to show the strength and significance of the association between each independent and dependent variable. A P-value less than 0.05 was used as a significant association.
Result
Socio-Demographic Characteristics of Participants
From five primary schools, 534 students were participating with a response rate of 100%. Males were 227 (42.5%). Of them, 91 (17.0%) grade five, 159 (29.8%) grade six, 139 (26.0%) grade seven and 145 (27.2%) eight. The student’s minimum age was 9 and the maximum 22 years. The mean and standard deviation of age was 14.34± 1.56 years (Table-1).
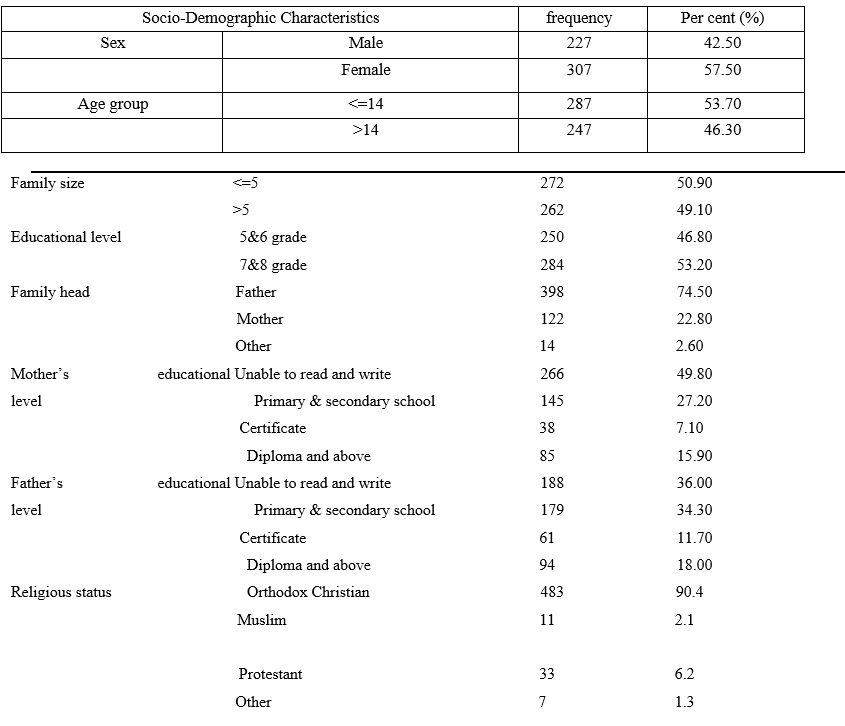
Table 1: Socio-Demography of Participants in Fiche town, Oromia, Central, Ethiopia, 2022 (N=534).
*Other (wake feta, non-religious)
Knowledge on Oral Hygiene
The student had good knowledge 449 (84.1%). Almost all (95.1%) student educated about oral hygiene. From family 332 (65.4%), from teachers 281(55.3), from health worker 149 (29.3%), from media 132 (26%) and school clubs108 (21.3%) (Table-2).
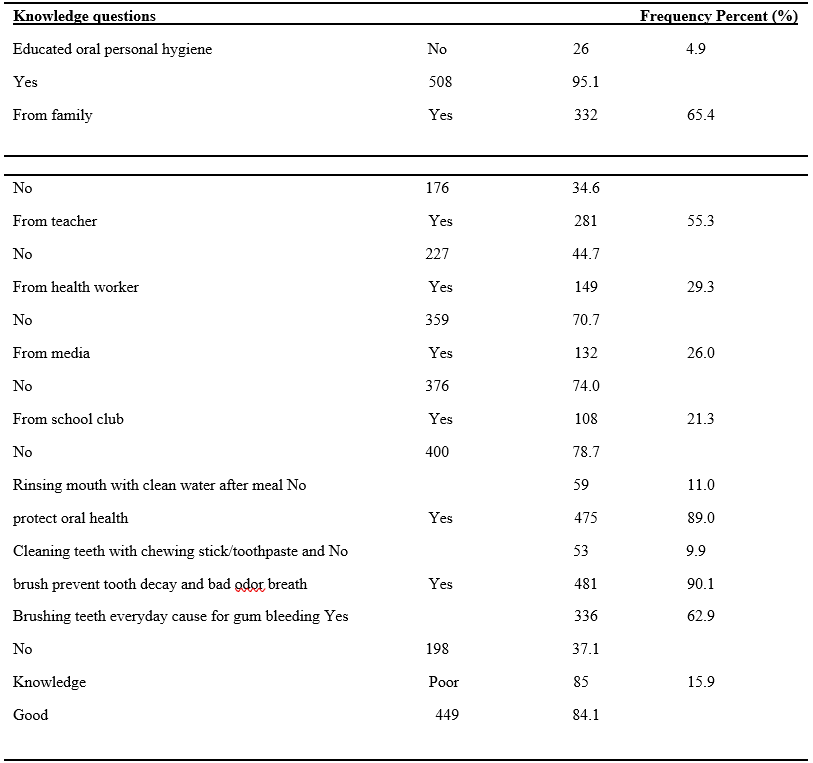
Table 2: shows knowledge towards oral hygiene practice among students of Participants in Fiche town, Oromia, Central, Ethiopia, 2022 (N=534).
Magnitude on Oral Hygiene Practices
The good oral hygiene practices of students were 295 (55.2%) (Fig:2). About 472 (88.4%) of students brush their teeth but brush every day 357 (66.9%) and twice per day 147 (27.5%). The recommended practice of students, whose duration of the toothbrush was less than60 seconds was256 (47.9%) and around 146 (27.3%) of students used traditional sticks to brush their teeth. The number of students who were seen by a dentist was 407 (76.2%), but only 43 (8.1%) were having regular checkups (Table-3).

Figure 2: The magnitude of oral hygiene practice among Student Fiche Town, Oromia, Ethiopia, 2022.
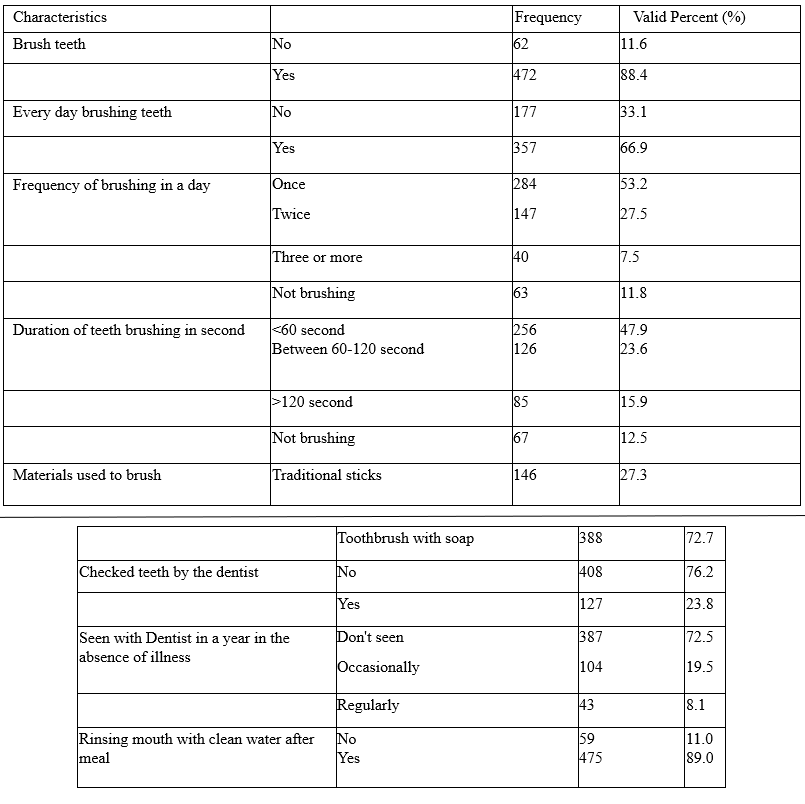
Table 3: Magnitude on Oral hygiene practices of Participants in Fiche town, Oromia, Central, Ethiopia, 2022 (N=534).
Factors Associated with Oral Hygiene Practice
The association of different factors with oral hygiene was assessed by simple logistic regression analysis and displayed in odds ratio [95% confidence interval (CI)]. Under sociodemographic characteristics. The student’s mother educational status [crude odds ratio (COR): 2.84, 95% CI (1.21, 6.66); P=.017) were certifiable and (COR: 1.93, 95% CI (1.10, 3.38); P=.022) diploma and above. The student’s father’s educational status primary and secondary school were diploma and above were (COR; 2.11, 95% CI (1.20, 3.70); P= .010).
The student’s mother who were governmental employees (COR: 3.19, 95% CI (1.68, 6.09); P=.000), were merchant (COR: 2.03, 95% CI (1.07, 3.85); P=.030), mother who were house wife were (COR: 2.12, 95% CI (1.22, 3.69); p=. 008), father governmental employees (COR: 2.49, 95% CI (1.51, 4.10); p=.000) and merchant (COR: 1.81,95% CI (1.06, 3.11); P=.031).
The students were member of school health related clubs were (COR: 1.93, 95% CI (1.28, 2.90); p=.002). There was school personal hygiene inspection had (COR: 2.51, 95%CI (1.70, 3.71); p=.000) and had trained at school on personal hygiene (COR: 1.73, 95% CI (1.23, 2.44); p=.008) were crudely associated with good oral hygiene practice.
In final multivariable analysis, under multilevel logistic regression, after adjusting for the potential confounders: being female (adjusted odds ratio (AOR): 1.64, 95% CI (1.08, 2.49); p=.02), the student’s mother, whose occupation was homemaker (AOR: 2.09, 95% CI (1.07, 4.10); p=.01), and school personal hygiene inspection (AOR: 2.47, 95% CI (1.54, 3.97) ; p=.00) were significantly associated with good oral hygiene practice (Table-4).
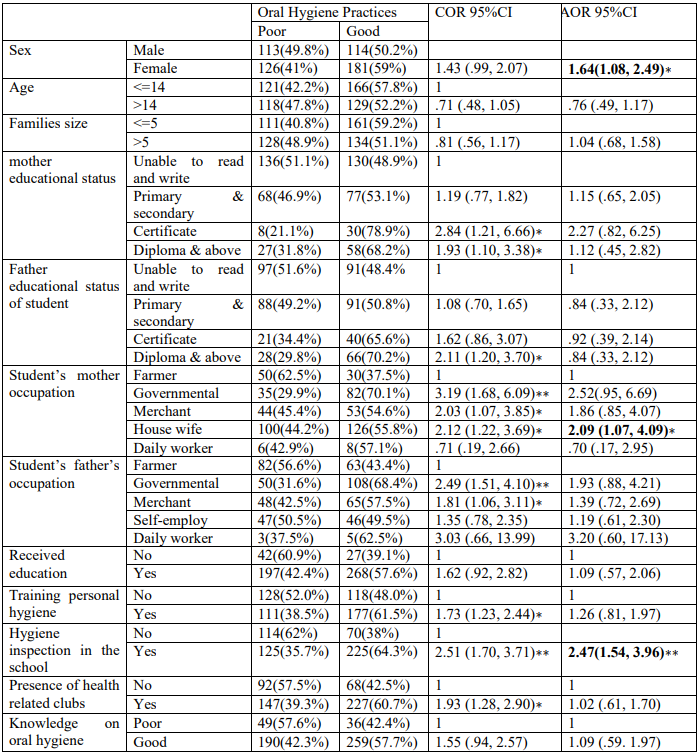
Table 4: Factors Associated with Oral Hygiene Practice of students in Fiche town, Oromia, Ethiopia, 2022 (N=534).
Key: - COR (Crude Odd Ratio), AOR (Adjusted Odd Ratio) ∗ 𝑃 – 𝑣𝑎𝑙𝑢𝑒 < .05 And ∗∗ 𝑝 – 𝑣𝑎𝑙𝑢𝑒 < .001
Discussion
This study assesses the determining the extent to which oral hygiene practices among students. oh was influenced by various circumstances. Poor oral hygiene can result in dental caries, gingivitis, periodontitis, tooth loss, bad breath (halitosis), fungal infections, and various gum diseases [2]. Almost half 239 (44.8%) of students had poor oral hygiene practice; 284 (53.2%) of the students were brushed once a day; 147 (27.5%) twice per day morning and night. This result was smaller than research done in Alem Ketema has 70% once a day and 30% twice a day brush their teeth [10]; this may be due to the large sample size used and 74.1% once and 18.8 % twice a day brushed in rural Communities, Southwest Nigeria [13]. This may be due to parental educational status.
The majority of students, 475 (89%) were rinsing their mouth with clean water after meals; this was higher in Alem Ketema, 55.3% [10] and in Bangladesh, 24.7%. This may be due to the sample size and study area [8]. Around 146 (27.3%) students were using toothpick/stick to clean interdental areas. This isn’t good cleaning the interdental areas of the tooth when compared with dental floss [8]. Twelve (2.2%) flossing was used for interdental cleaning. This result is very low compared with the research done in Fiche secondary school, 83.3% [14]; this was due to the difference in educational level and age of students. 62% of Bangladesh’s primary schools used a toothpick or stick for interdental cleaning [8]. One hundred fourth six (27.3%) used traditional sticks as brushing material and 63 (11.8%) never brushed their teeth. This result was smaller, 67.6% used sticks in Bahardar City [15], almost similar to the 9.7% of students who had never brushed their teeth in Southeast, Nigeria [16].
Nearly one-third of students 387 (72.5%) had never seen a dentist. This result is smaller than research done 83% of Fiche Preparatory School Students in Fiche Town, Oromia, Ethiopia [14], and 92.8% in South‑East Nigeria [16], this difference may be because of the setting area was a town. The knowledge of the student prevalence of oral hygiene was 449 (84.1%); this result was higher at 59.42% in Guangzhou [17], no reason.
The students who are female are 1.64 times more likely to have good oral hygiene than males; this result was supported by research done in South West Nigeria female1.38 [13], 1.33 in Southcentral Alaska, India [18]. The student’s mother’s occupation status was homemaker, and she had 67.6% more likely to have good oral hygiene compared with the student’s mother’s occupational status was farmed, governmental, or merchant. This may be due to not having enough time to take care of their children. The presence of hygiene inspection was 2.47 times more likely to have good oral hygiene practice compared with non-inspection in school.
Conclusion
Overall, good OP among primary school children in Fiche Town was low. Female sex student, the student’s mother’s occupation was a homemaker and had school hygiene inspections was associated with good OP.
Recommendation
Schools, health extension workers, and families are recommending raising students’ oral hygiene practice through health education, training, and hygiene inspection in a way that could lead to good oral hygiene practice. In addition, I am recommended to stakeholders (school directors, school supervisors, teachers, and families) collaborate to ensure the student’s hygiene practices. Further study can make to quantify factors of oral hygiene that were not addressed in our study: wealth index, diet taking, substance use, and dental caries.
Declaration
Ethical Approval and Consent of Participants
Ethical approval obtained from the Institutional Review committee (IRC) with reference number 878/2022 of Salale University on March 20, 2022, E.C. Permission letter written by Salale University, College of Health Sciences provided to Fiche town educational office and each selected school to obtain permission. Written informed consent obtained from all students family consent (Assent) consent was taken from students who were younger than 18 years. Any information recorded anonymously and confidentially.
Consent for Publication: Not applicable
Availability of Data and Material: All data including this study were available with correspondence authors.
Conflicts of Interest: The authors declare that they have no conflicts of interest.
Funding: This study was partial funded by Salale University.
Acknowledgement
We would like to acknowledge the contribution all the students, teacher, parents, Fiche Town educational office and data collectors for their cooperation and participation in the study, without them, the study would not have been possible.
References
- Divine-Favour Chichenim Ofili. “Oral hygiene practices and utilization of oral healthcare services among in-school adolescents in,” Pan Afr. Med J. 2020;36:300. [PubMed.]
- SA Sheth., PJ Dhaduk., R Siddhi., and MR Jogi. “Oral Hygiene Practices and Factors Affecting. Oral Health Service Utilization among Children (11 – 14 Years) of Government School of Nikol Ward of East Zone of Ahmedabad, Gujarat, India. 2019;10(2):299-303. [PubMed.]
- SA Saadaldina., et al. “Awareness and Practice of Oral Health Measures in Medina, Saudi Arabia: An Observational Study. 2020;17(23):9112. [Ref.]
- FA Ahmad., MK Alotaibi., M Abdul., and B Sanaa. “The Effect of Oral Health Knowledge, Attitude, and Practiceon Periodontal Status among Dental Students. 2019;1-7. [PubMed] [PubMed.]
- T Tefera., et al. “Dental health problems and treatment ‑ seeking behavior among special need school students in Amhara region. Ethiopia. 2021;1-9. [PubMed.]
- D Fukuhara., et al. “Relationship between oral hygiene knowledge, source of oral hygiene knowledge and oral hygiene behavior in Japanese university students: A prospective cohort study. 2020;15(7):1-13. [PubMed.]
- F Hua., et al. “Oral hygiene care for critically ill patients to prevent ventilator- associated pneumonia. 2016;10. [PubMed.]
- A Bhuiyan., H B Anwar., RB Anwar., and M N Ali. “Oral Hygiene Awareness and Practices among a Sample of Primary School Children in Rural Bangladesh. 2020;8(36):1-9. [PubMed] [PubMed.]
- SAH Jouhar., R Ahmed., MA Khurshid., Z Bokhari. “Association of BMI, Diet, Physical Activity, and Oral Hygiene Practices with DMFT Index of Male Dental Students at King Faisal University, Al-Ahsa. 2021;13(224):1-15. [PubMed] [PubMed.]
- A Shitie., R Addis., A Tilahun., and W Negash. “Prevalence of Dental Caries and Its Associated Factors among Primary School Children in Ethiopia. 2021;7. [Ref.]
- Y Tafere., S Chanie., T Dessie., and H Gedamu. “Assessment of prevalence of dental caries and the associated factors among patients attending dental clinic in Debre Tabor general hospital: a hospital-based cross- sectional study. 2018;1-7. [PubMed.]
- Y Fukuya., Y Matsuyama., A Isumi., S Doi., and M Ochi. “Toothbrushing and School Refusal in Elementary School: A Longitudinal Study. 2020;8-10. [PubMed.]
- CA Akinyamoju., DM Dairo., I A Adeoye., and AO Akinyamoju. “Dental Caries and Oral Hygiene Status: Survey of School children in Rural Communities, Southwest Nigeria. 2018;25(4):239-245. [PubMed.]
- R Shukure and D Shuke. “Assessment of Knowledge and Practice on Oral Health and Oral Hygiene Status Among Fitche Preparatory School Students in Fitche Town, Oromia, Ethiopia. 2018;3(6):30-34. [Ref.]
- W Mulu., T Demilie., M Yimer., K Meshesha., and B Abera. “Dental caries and associated factors among primary school children in Bahir Dar city: a cross-sectional study. 2014;7(949):1-7. [PubMed.]
- NK Onyejaka., O O Olatosi., NA Ndukwe., EO Amobi. “Prevalence and Associated Factors of Dental Caries among Primary School Children in South‑East Nigeria. 2021;24:1300-1306. [PubMed] [PubMed.]
- N Pan., L Cai., C Xu., H Guan., and Y Jin. “Oral health knowledge, behaviors and parental practices among rural – urban migrant children in Guangzhou a follow-up study. 2017;17:97:1-11. [PubMed.]
- VY Hiratsuka. “Oral health beliefs and oral hygiene behaviours among parents of urban Alaska Native children. 2019;78(1). [PubMed.]