>Corresponding Author : Andrew S Ryser
>Article Type : Technique Article
>Volume : 4 | Issue : 3
>Received Date : 30 May, 2024
>Accepted Date : 11 June, 2024
>Published Date : 15 June, 2024
>DOI : https://doi.org/10.54289/JDOE2400113
>Citation : Ryser AS, Sabol JV, Handel SE, McLaughlin S, Johnson TM, et al (2024) Digital Workflow for Interdisciplinary Communication in Crown Lengthening Surgery. J Dent Oral Epidemiol 4(3): doi https://doi.org/10.54289/JDOE2400113
>Copyright : © 2024 Ryser AS, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Technique Article | Open Access | Full Text
1Resident, Department of Prosthodontics, Army Postgraduate Dental School, Postgraduate Dental College, Uniformed Services University, Fort Eisenhower, GA, USA
2Program Director, Department of Prosthodontics, Army Postgraduate Dental School, Postgraduate Dental College, Uniformed Services University, Fort Eisenhower, GA, USA
33Assistant Program Director, Department of Prosthodontics, Army Postgraduate Dental School, Postgraduate Dental College, Uniformed Services University, Fort Eisenhower, GA, USA
44Program Director, Department of Prosthodontics, Army Postgraduate Dental School, Postgraduate Dental College, Uniformed Services University, Fort Eisenhower, GA, USA
55Resident, Department of Prosthodontics, Army Postgraduate Dental School, Postgraduate Dental College, Uniformed Services University, Fort Eisenhower, GA, USA
*Corresponding author: Andrew S Ryser, Prosthodontic Resident, CPT, Department of Prosthodontics, Army Postgraduate Dental School, Postgraduate Dental College, Uniformed Services University, Fort Eisenhower, GA, USA
Abstract
When planning a prosthetic rehabilitation in the maxillary anterior, crown lengthening surgery is frequently indicated to adjust the position of the gingival margin and expose sufficient tooth structure for an ideal restoration. A surgical template can be used to prescribe the ideal postsurgical gingival architecture. However, producing a template that both seats onto the existing dentition and relates the desired gingival margin position is a clinical challenge. The digital workflow presented in this report employs a hybrid model merging the pre-prosthetic coronal tooth structure with the proposed postsurgical gingival margins. Using this model, the 3D printed surgical guide facilitates precise crown lengthening of the maxillary dentition.
Keywords: Digital Dentistry, 3D printing, crown lengthening, surgery, diagnostic
Abbreviations: CAD: Computer Aided Design, PMMA: Polymethyl Methacrylate, CAD-CAM: Computer Aided Design- Computer Aided Manufacturing
Introduction
Crown lengthening is defined by the American Academy of Periodontology as a surgical procedure that aims to expose sound tooth structure for restorative purposes via apical repositioning of the gingival tissue with or without removal of alveolar bone [1]. Crown lengthening can be further classified as functional or esthetic [2]. Functional crown lengthening facilitates restoration of teeth exhibiting inadequate coronal tooth structure or avoids violation of the supracrestal tissue attachment [3]. Esthetic crown lengthening is performed to remove excess gingiva and expose tooth structure for esthetic reasons with or without osseous resection [4]. The need for crown lengthening may arise through developmental (e.g. gingival excess) or acquired (e.g. caries, dental fracture) processes [2]. The diagnostic wax-up is used to determine the feasibility of a proposed treatment plan, to assess possible esthetic outcomes, and determine the desired occlusal and functional relationships of the dentition. The diagnostic wax up can also be a guide for surgical treatment goals [5]. For the surgeon, the wax-up communicates the planned tooth extractions, the positions of dental implants, the ideal gingival margin location, and possible areas of osseous reduction [6]. Prior to crown lengthening surgery, the wax-up can be used to create a surgical template that prescribes the desired final gingival margin position [7]. Traditionally, diagnostic wax-ups were completed by applying wax onto stone casts. However, diagnostic wax-ups can now be generated using a digital workflow. Upon completion of the digital wax-up the clinician can print the diagnostic model to fabricate a surgical template, or the clinician can design a surgical guide digitally and print the guide prior to surgery. The purpose of this report is to demonstrate a fully digital pathway for precise interdisciplinary communication relating the pre-existing dentition to the final gingival margin position.
Materials And Methods
A 65-year-old female presented to a prosthodontics practice with partial edentulism and mild to moderate wear of the remaining dentition (Fig.1). The patient’s chief complaint was related to the poor esthetics in the maxillary anterior region. The patient exhibited clinical gingival health on an intact periodontium. Inconsistent gingival margins secondary to dentoalveolar extrusion were noted. Treatment options were presented and patient elected to have esthetic crown lengthening in the maxillary anterior region followed by delivery of fixed and removable prostheses. The patient consented to all treatment after written and verbal counseling.
Diagnostic impressions of the maxillary and mandibular arches were made with irreversible hydrocolloid. The impressions were poured, trimmed, and scanned using Primescan (Dentsply Sirona, USA). A digital wax-up was completed using computer-aided design (CAD) software (exocad DentalCAD, exocad, Darmstadt, Germany) (Fig. 2). The original cast and the digital wax-up model were merged to permit surgical template fabrication. The hybrid cast reflected the gingival margin locations established by the digital wax-up yet retained the morphology of the unprepared teeth (Fig. 3). Thus, the surgical template designed using the hybrid cast seated on unprepared teeth and accurately communicated the planned gingival margin location to the surgeon (Fig. 4). The surgical guide was printed in surgical guide resin (Surgical Guide Resin, Formlabs, Somerville, MA, USA), washed, cured, and finished.
The printed surgical template was used during crown lengthening surgery to transfer the desired gingival margin position to the patient. Following gingivectomy and full-thickness flap reflection, osteoplasty and ostectomy were performed to place the alveolar crest 3mm apical to the desired gingival margin, establishing the proper supracrestal attached tissue dimension and minimizing rebound during healing (Fig. 5) [8-10]. After 6 months, the teeth were prepared for crowns and provisionalized with milled PMMA restorations (Telio CAD, Ivoclar Vivadent, Schaan, Liechtenstein) (Fig. 6).
Discussion
The purpose of this report was to present a digital workflow for transferring planned gingival margin positions to the patient during multidisciplinary rehabilitation of the maxillary anterior dentition. In such cases, optimizing clinical and patient-centered treatment outcomes relies heavily on accurate and effective communication between surgical and restorative team members.11 Any miscommunication between dentists can lead to a compromised treatment plan and a negative experience for the patient [11]. The diagnostic wax-up is a laboratory procedure completed to communicate the proposed treatment plan not only from the laboratory to the restoring dentist, but to other dentists involved in the patient’s care. The Glossary of Prosthodontic Terms defines a diagnostic waxing as a waxing of intended restorative contours on dental casts for the purpose of evaluation, planning restorations, and establishing a wax replica of a proposed treatment plan [12].

Figure 1: Baseline appearance of the patient’s smile.
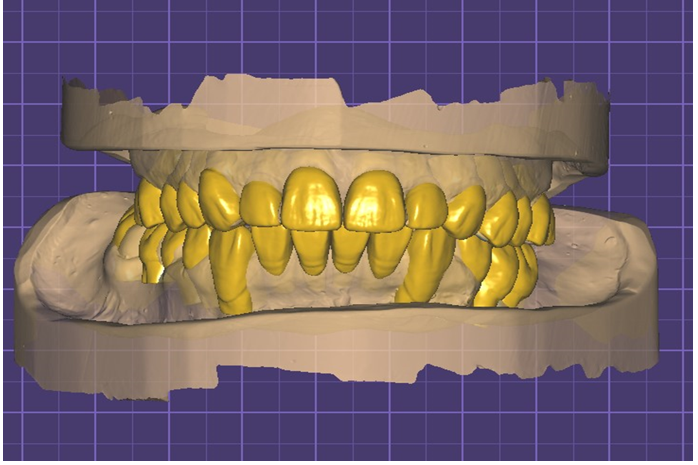
Figure 2: Digital wax-up in exocad.
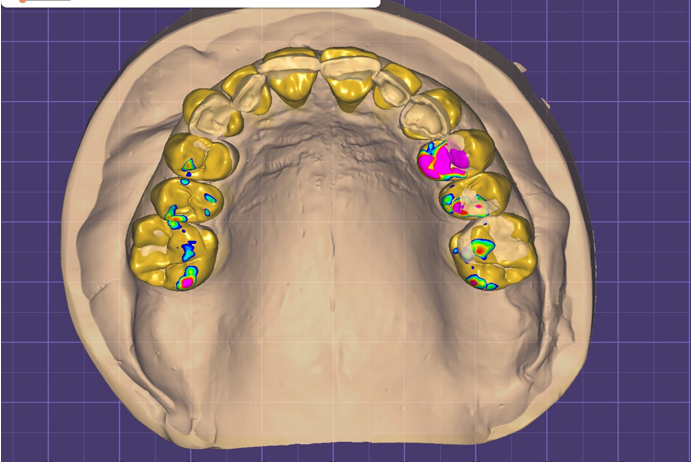
Figure 3: The digital wax-up and the scan of the diagnostic cast were merged to form a hybrid cast. The hybrid cast incorporated the desired final gingival margin position but retained the morphology of the unprepared maxillary teeth.
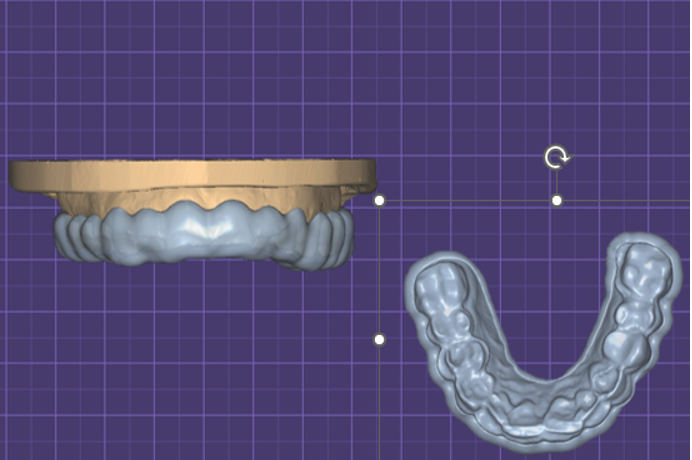
Figure 4: Surgical template for crown lengthening procedure. The surgical template fully seated on the patient’s baseline dentition but accurately related the desired gingival margin position to the surgeon.

Figure 5: Initial incisions demonstrating transfer of the planned gingival margin position to the patient.

Figure 6: Six months following crown lengthening. The maxillary teeth are provisionalized with milled PMMA crowns.
Conventionally, a diagnostic wax-up was completed by making diagnostic impressions, pouring to form stone casts, mounting the casts on an articulator, and then using wax and hand instruments to modify the contours of the teeth and gingiva. The esthetics and occlusion of the proposed restorations were set to ideal, and once completed, the wax-up could be used for communication among treatment team members—including the patient and the laboratory—as well as fabrication of provisional or final restorations [13]. Over the last two decades, digital workflows have replaced many analog processes in dentistry. Dental practitioners have increasingly utilized virtual diagnostic wax-ups and computer-aided design and manufacturing (CAD/CAM) [14]. Currently, high-quality digital wax-ups can be efficiently established utilizing computer software. Once completed, the digital file can be displayed on a computer screen, or a 3D model can be printed.
This digital file or printed model can have numerous clinical and educational applications. The proposed treatment plan can be presented to the patient, demonstrating potential esthetic and functional improvements. Using Digital Smile Design, the wax-up can be integrated into the patient’s smile, deepening the patient’s understanding of treatment plan [15]. The diagnostic proposal can then be sent to the oral surgeon or periodontist to aid in surgical planning [16]. Once the treatment plan is accepted by the patient and all clinicians involved, the lab can use the diagnostic wax-up to make provisional restorations for the restoring dentist [17]. Furthermore, the lab can fabricate surgical templates to guide precise adjustments to hard and soft tissue contours and accurately transfer planned implant positions [18].
In crown lengthening, producing a surgical template to communicate ideal gingival margins leads to an efficient, predictable, and reproducible procedure that facilitates a highly esthetic outcome [15]. Traditionally, surgical guides have been made using a vacuum-formed matrix over a duplicated cast of a diagnostic wax-up [19]. Digital technology in widespread use now permits designing high quality surgical templates directly from the digital wax-up. In a study by Li et al. (2024), the authors concluded that crown lengthening surgery performed using a 3D printed guide was more accurate than performing “free hand” surgery without a guide [20]. Digital templates are more predictable and can shorten surgery time when compared to the traditional vacuuform guides [21,22].
Summary
In multidisciplinary reconstruction of the maxillary anterior, diagnostic wax-ups are essential for idealizing function and esthetics. High quality digital wax-ups with numerous clinical and educational applications are easily produced and readily modifiable when adjustments are necessary. In this report, a digital workflow was presented for producing a crown lengthening template that seated on the patient’s baseline dentition yet related the planned gingival margin position to the surgeon. The presented workflow can be adapted to simplify numerous types of surgery involving resection of hard and soft tissue, dental implant placement, and implant site development.
Disclaimer: The views expressed in this manuscript are those of the authors and do not necessarily reflect the official policy of the United States Government, the Department of Defense, the Defense Health Agency, or Uniformed Services University.
Conflict of interest statement: The authors report no financial, economic, or professional interests that may have influenced the design, execution, or presentation of this work.
Acknowledgments: This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. The authors report no conflicts of interest.
References
- Glossary of Periodontal Terms. AAP Connect. (2024). [Ref.]
- Majzoub ZAK., Romanos A., Cordioli G. Crown lengthening procedures: A literature review. Semin Orthod. 2014;20(3):188–207. [Ref.]
- Alrmali A, Melker D, Zalucha J, Wang HL. Biological shaping as a conservative alternative for crown lengthening: A review. Clin Exp Dent Res. 2024;10:e873. [PubMed.]
- Petrutiu S. Esthetic crown lengthening – a link between Orthodontics and prosthetics. 2018. [Ref.]
- Simon H, Magne P. Clinically Based Diagnostic Wax-up for Optimal Esthetics: The Diagnostic Mock-up. J Calif Dent Assoc. 2008;36(5):355-362. [PubMed.]
- Villalobos-Tinoco J, Jurado CA, Rojas-Rueda S, Fischer NG. Additive Wax-Up and Diagnostic Mockup As Driving Tools for Minimally Invasive Veneer Preparations. Cureus. 2022;14:e27402. [PubMed.]
- Gomes S, Matarredona Á, Barrachina T, Deliberador TM, Stefani A. Importance of the Diagnostic Wax-up When Planning a Periodontal Surgical Guide in Esthetic Surgery. PubMed. 2023;44:142-6. [PubMed.]
- Ingber JS, Rose LF, Coslet JG. The "biologic width"--a concept in periodontics and restorative dentistry. Alpha Omegan. 1977;70:62-65. [PubMed.]
- Lanning SK, Waldrop TC, Gunsolley JC, Maynard JG. Surgical crown lengthening: evaluation of the biological width. J Periodontol. 2003;74:468-474. [PubMed.]
- Brägger U, Lauchenauer D, Lang NP. Surgical lengthening of the clinical crown. J Clin Periodontol. 1992;19:58-63. [PubMed.]
- Ismail EH, Al-Moghrabi D. Interrelationship between dental clinicians and laboratory technicians: a qualitative study. BMC Oral Health. 2023;23:682. [PubMed.]
- The glossary of prosthodontic terms. Tenth Edition. J Prosthet Dent. 2023;130:e7-e126. [PubMed.]
- Chisnoiu AM, Staicu AC, Kui A, Chisnoiu RM, Iacob S, Fluerașu M, Buduru S. Smile Design and Treatment Planning-Conventional versus Digital-A Pilot Study. J Pers Med. 2023 Jun;13:1028. [Ref.]
- Segundo ART, Saraiva S, de Castro C, Sesma N, Bohner L, Andretti FL, Coachman C. CAD-CAM natural restorations-Reproducing nature using a digital workflow. J Esthet Restor Dent. 2023. 35(7):993-1000. [PubMed.]
- Thomas PA, Krishnamoorthi D, Mohan J, Raju R, Rajajayam S, Venkatesan S. Digital Smile Design. J Pharm Bioallied Sci. 2022;14:S43-S49. [Ref.]
- Chen P, Nikoyan L. Guided implant surgery: a technique whose time has come. Dent Clin North Am. 2021;65:67-80. [PubMed.]
- Sergiu D, Viorel P, Costea R, Oana E, Mihai B, Raluca M, et al. Diagnostic Wax-Up - an extremely important method of communication between the dental office and the dental laboratory. Rom J Med Pract. 2022;17:66-71. [Ref.]
- Alhumaidan A, Al-Qarni F, AlSharief M, AlShammasi B, Albasry Z. Surgical guides for esthetic crown lengthening procedures. J Am Dent Assoc. 2021;153:31-38. [PubMed.]
- Malik K, Tabiat-Pour S. The Use of a Diagnostic Wax Set-up in Aesthetic Cases involving Crown Lengthening – A Case Report. Dent Update. 2010;37:303-307. [PubMed.]
- Li Y, Liu M, Zhou T, Lyu J, Tan J, Liu X. Accuracy of three types of digital guides for Crown lengthening surgery: An in vitro study. J Dent Sci. 2024;19:39-45. [PubMed.]
- Andrade N, Moura G, Maska B, Kaigler D, Mendonça G, Wang H. Dual digitally guided crown lengthening in esthetic area compromised by disharmonic implant Crown. Clin Adv Periodontics. 2021;12:26-31. [PubMed.]
- Alazmi SO. Three dimensional digitally designed surgical guides in esthetic crown lengthening: A clinical case report with 12 months follow up. Clin Cosmet Investig Dent. 2022;14:55-59. [PubMed.]