>Corresponding Author : Sahel Imane
>Article Type : Case Report
>Volume : 6 | Issue : 2
>Received Date : 02 April, 2026
>Accepted Date : 11 April, 2026
>Published Date : 11 May, 2026
>DOI : https://doi.org/10.54289/JCRMH2600109
>Citation : Ezahraa TF, Imane S, Asmae D, Intissar S, Benchrifi Y, et al. (2026) Primary Large Cell Neuroendocrine Carcinoma of the Breast: A Case Report and Literature Review. J Case Rep Med Hist 6(2): doi https://doi.org/10.54289/JCRMH2600109
>Copyright : © 2026 Ezahraa TF, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Case Report | Open Access | Full Text
1Medecin resident, Service de gynecologie-obstetrique, CHU Ibno Rochd, Casablanca, Marocco
2Professeur au Service de gynecologie-obstetrique, CHU Ibno Rochd, Casablanca, Marocco
*Corresponding author: Sahel Imane, Medicine resident, Service de gynecologie-obstetrique, CHU Ibno Rochd, Casablanca, Morocco
Abstract
Primary neuroendocrine neoplasm of the breast (PNENB) is a rare subtype of breast cancer, accounting for <1% of all breast tumors [1]. They are subclassified into well-differentiated and poorly differentiated neuroendocrine tumors, as well as invasive breast carcinoma with neuroendocrine features. Well-differentiated tumors show architectural similarity to carcinoids of other sites but lack characteristic neuroendocrine nuclei [2]. A definitive diagnosis relies on histological and immunohistochemical examinations, with neuroendocrine differentiation requiring expression of synaptophysin or chromogranin. The main differential diagnosis is metastatic neuroendocrine tumor from an extramammary site. Neuroendocrine tumors of the breast are treated similarly to other invasive breast carcinomas [2]. Due to the low incidence and limited research on primary NETs, accurate diagnosis, selection of specific treatment options, and determination of long-term prognosis remain significant challenges in managing this rare form of breast cancer [3].
Abbreviations: PNENB: Primary Neuroendocrine Neoplasm of the Breast, WHO: World Health Organization, TTF: Thyroid Transcription Factor, NEN: Neuroendocrine Neoplasms, NEC: Neuroendocrine Carcinoma, NET: Neuroendocrine Tumors, NEC: Neuroendocrine Carcinomas, IBC-NST: Invasive Breast Carcinoma of No Special Type, NEDCIS: Neuroendocrine Ductal Carcinoma In Situ, NEBC: Neuroendocrine Breast Cancer, IDC-NST: Invasive Ductal Carcinoma of No Special Type
Introduction
Neuroendocrine tumors of the breast represent a rare and heterogeneous subgroup of breast malignancies. First described in the literature in the 1970s, these tumors share histological and immunohistochemical features with neuroendocrine tumors arising in the gastrointestinal tract and lungs. The World Health Organization (WHO) classifies breast neuroendocrine neoplasms into well-differentiated neuroendocrine tumors, poorly differentiated neuroendocrine carcinomas (including small cell carcinoma), and invasive breast carcinomas with neuroendocrine differentiation. The pathogenesis of these tumors remains poorly understood, although it is hypothesized that they arise from the differentiation of neoplastic epithelial cells rather than from native neuroendocrine cells in the breast [3-5].
Case Report
A 70-year-old woman was admitted to Ibn Rochd University Hospital on December 31, 2024, presenting with a left breast mass that had been evolving for more than one month. Clinical examination revealed an inflammatory left breast with a large mass occupying nearly the entire breast. No palpable axillary lymphadenopathy was identified.
Breast ultrasound performed on October 14, 2025, demonstrated a large hypoechoic and heterogeneous mass located at the junction of the lower inner quadrants of the left breast, measuring 4.2 × 4.5 cm. The lesion exhibited irregular margins without posterior acoustic attenuation. Additional findings included right-sided ductal ectasia with echogenic content.
Bilateral axillary lymph nodes were subcentimetric, oval in shape, and displayed preserved fatty hila, suggestive of reactive changes. The lesion was classified as BI-RADS 4 according to the American College of Radiology (Fig 1).
A core needle (Tru-Cut) biopsy was subsequently performed. Histopathological examination revealed multiple cores of breast parenchyma infiltrated by a poorly differentiated invasive tumor proliferation with extensive necrosis. The tumor was composed of sheets of markedly atypical (anisokaryotic) cells with eosinophilic cytoplasm and irregular hyperchromatic nuclei with prominent nucleoli. Mitotic activity was high, estimated at 22 mitoses per 2 mm². No glandular differentiation or intraductal component was identified. The stroma showed a moderate fibro-inflammatory reaction with focal myxoid changes. Adjacent breast tissue exhibited ductal ectasia and simple ductal hyperplasia.
Immunohistochemical analysis demonstrated that tumor cells were positive for cytokeratin AE1/AE3, while negative for mammaglobin and GATA3 (with appropriate internal controls). Neuroendocrine markers CD56 and synaptophysin were positive, whereas chromogranin was negative. Tumor cells did not express estrogen or progesterone receptors. The Ki-67 proliferation index was markedly elevated, approaching 100%. Thyroid transcription factor-1 (TTF-1) expression was negative.
Overall, the morphological and immunohistochemical findings were consistent with a diagnosis of large cell neuroendocrine carcinoma of the breast. Given the clinical presentation of carcinomatous mastitis, the patient was referred to the oncology department to initiate neoadjuvant therapy.
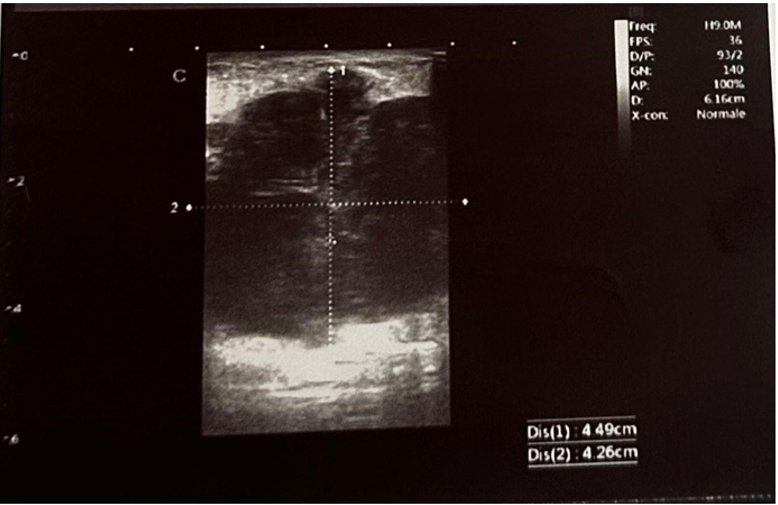
Figure 1.
Neuroendocrine neoplasms (NENs) represent a heterogeneous group of tumors defined by predominant neuroendocrine differentiation, encompassing both well-differentiated and poorly differentiated forms. NENs of mammary origin are exceptionally rare, accounting for less than 1% of all NENs and exhibiting a reported incidence ranging from 0.1% to 20% among breast cancers [6]. The diagnosis of primary neuroendocrine breast tumors is challenging and remains one of exclusion, requiring thorough evaluation to rule out metastatic disease from extramammary primary sites.
From a clinical and radiological standpoint, neuroendocrine carcinoma (NEC) of the breast lacks specific distinguishing features, making histopathological and immunohistochemical analyses essential for definitive diagnosis [4]. These tumors are believed to arise from neuroendocrine differentiation within conventional breast carcinoma. According to the 2012 World Health Organization classification, breast neuroendocrine neoplasms were categorized into three subtypes [5]. The updated 2019 classification introduced a more standardized framework, defining NENs as tumors with predominant neuroendocrine differentiation and subdividing them into well-differentiated neuroendocrine tumors (NETs), poorly differentiated neuroendocrine carcinomas (NECs), and invasive breast carcinoma of no special type (IBC-NST) with neuroendocrine differentiation. Importantly, the diagnosis of NEN is reserved for tumors in which more than 90% of cells exhibit neuroendocrine features, whereas tumors with partial differentiation are classified as IBC-NST with neuroendocrine features [7].
Clinically, neuroendocrine breast tumors often present similarly to conventional breast carcinomas; however, certain features such as bloody nipple discharge have been reported. This manifestation has been associated with neuroendocrine ductal carcinoma in situ (NEDCIS), which may represent a preinvasive precursor of invasive neuroendocrine tumors [7]. In addition, neuroendocrine breast cancer (NEBC) may demonstrate a higher likelihood of distant metastasis at diagnosis compared to invasive ductal carcinoma of no special type (IDC-NST), despite sharing overlapping clinical characteristics [8]. Most cases express estrogen and progesterone receptors, suggesting a luminal-like phenotype.
Diagnosis relies primarily on histopathological examination supported by immunohistochemical detection of neuroendocrine markers, particularly chromogranin A and synaptophysin, which remain the most sensitive and specific indicators of neuroendocrine differentiation [9]. Despite advances in diagnostic criteria, the rarity and heterogeneity of these tumors continue to pose significant challenges in both classification and management.
Conclusion
Large cell neuroendocrine carcinoma of the breast is an extremely rare and aggressive subtype of breast cancer. Its clinical and radiological features are largely non-specific, rendering histopathology and immunohistochemistry essential for definitive diagnosis. Neuroendocrine markers such as CD56 and synaptophysin are crucial for confirming neuroendocrine differentiation, while exclusion of metastatic disease is mandatory. Due to the high proliferative index and potential for rapid progression, early recognition and timely initiation of systemic therapy are critical. Given the scarcity of cases, standardized treatment protocols are lacking, and management is largely extrapolated from conventional breast carcinoma guidelines. Reporting additional cases is essential to enhance understanding of tumor biology, optimize therapeutic strategies, and improve prognostic assessment.
References
- Santoro A., Mule A., Rossi ED., et al. Neuroendocrine neoplasms of the breast: a review of literature. Virchows Arch. 2024;485(2):197–212. [PubMed.]
- El Arab KF., Bourhafour M., Elqasseh R., Khoaja A., et al. Primary neuroendocrine tumors of the breast: About a case and review of the literature. Int J Surg Case Rep. 2022;99:107642. [PubMed.]
- Ozaki Y., Miura S., Oki R. Neuroendocrine Neoplasms of the Breast: The Latest WHO Classification and Review of the Literature. Cancers (Basel). 2021;14(1):196. [PubMed.]
- Salemis NS. Primary neuroendocrine carcinoma of the breast: a rare presentation and review of the literature. Intractable Rare Dis Res. 2020;9(4):233–246. [PubMed.]
- Hasbay B., Ozgur Aytac H., Bolat FA. Neuroendocrine Tumors of the Breast: Single-Center Experience. J Clin Pathol. 2022;18(1):30-36. [PubMed.]
- Ozdirik B., Kayser A., Ullrich A., et al. Primary Neuroendocrine Neoplasms of the Breast: Case Series and Literature Review. Cancers (Basel). 2020;12(3):733. [PubMed.]
- Wang J., Wei B., Albarracin CT., et al. Invasive neuroendocrine carcinoma of the breast: analysis from SEER database. BMC Cancer. 2014;14:147. [PubMed.]
- Graca S., Esteves J., Costa S., et al. Neuroendocrine breast cancer. BMJ Case Rep. 2012;bcr122011534. [PubMed.]
- BMC Cancer retrospective studies on breast carcinomas with neuroendocrine features (incidence and diagnostic challenges). BMC Cancer. 2017;17:72. [Ref.]