>Corresponding Author : Chawki Khawla
>Article Type : Case Report
>Volume : 6 | Issue : 2
>Received Date : 28 April, 2026
>Accepted Date : 20 May, 2026
>Published Date : 28 May, 2026
>DOI : https://doi.org/10.54289/JCRMH2600108
>Citation : Khawla C, Saad A, Mehdi B, Salma F, Maha B, et al. (2026) Fatal Delay: How a Neurological Presentation Concealed Destructive Aortic Infective Endocarditis with Paravalvular Abscess. J Case Rep Med Hist 6(2): doi https://doi.org/10.54289/JCRMH2600108
>Copyright : © 2026 Khawla C, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Case Report | Open Access | Full Text
Ibn rochd university hospital, Casablanca, Morocco
*Corresponding author: Chawki Khawla, Ibn rochd university hospital, Casablanca, Morocco
Keywords: Infective Endocarditis; Aortic Valve; Paravalvular Abscess; Valve Perforation; Septic Embolism; Neurological Complications; Tetraparesis; Transesophageal Echocardiography; Delayed Diagnosis
Abbreviations: IE: Infective Endocarditis, TTE: Transthoracic Echocardiography, TEE: Transesophageal, MRI: Magnetic Resonance Imaging, CSF: Cerebrospinal Fluid, CTA: Computed Tomography Angiography
Introduction
Infective endocarditis (IE) is a serious infection of the endocardial surface of the heart, most often involving cardiac valves. Despite advances in microbiological diagnosis, multimodality imaging, and surgical techniques, IE continues to carry a 30-day mortality of 15–30% and an in-hospital mortality of up to 25% in contemporary cohorts [1,2]. Its incidence is estimated at 3–10 episodes per 100,000 person-years in high-income countries, with a notable shift in epidemiology toward older patients and nosocomial acquisition [3].
The clinical presentation of IE is notoriously heterogeneous. While fever, a new cardiac murmur, and peripheral stigmata of embolism represent the classic triad, a growing body of evidence highlights the frequency with which extracardiac — particularly neurological — manifestations dominate the initial presentation [4,5]. Neurological complications of IE, including ischemic stroke, transient ischemic attacks, meningitis, cerebral abscess, and hemorrhagic transformation, occur in up to 40% of patients with left-sided IE and are a leading cause of mortality and long-term morbidity [5,6]. When neurological symptoms overshadow cardiac manifestations, they may direct clinical evaluation away from the heart, leading to delayed diagnosis and missed therapeutic windows [7].
Echocardiography remains the cornerstone of IE diagnosis. However, transthoracic echocardiography (TTE) has a sensitivity of only 40–63% for vegetations in native valve IE, which drops further for early or small lesions [8]. Perivalvular complications — including abscess, pseudoaneurysm, fistula, and valve perforation — are detected with a sensitivity of only 28% by TTE, compared to 87% by transesophageal echocardiography (TEE) [9,10]. The 2023 ESC Guidelines for the Management of Endocarditis explicitly recommend TEE in all patients with suspected IE and a negative or non-diagnostic TTE, and advocate for its early use given its superior diagnostic accuracy [1].
We present a fatal case of aortic IE complicated by valve perforation, paravalvular abscess, and multifocal septic embolic strokes, in which the neurological presentation led to initial misattribution of the syndrome to a primary central nervous system infection. This case provides a compelling illustration of the diagnostic pitfalls of neurological IE and underscores the imperative of early, systematic echocardiographic evaluation in febrile patients with multifocal ischemic strokes.
Case Presentation
Presentation and Initial Neurological Assessment
A 62-year-old man with no known history of cardiac disease, valvular pathology, prior cardiac surgery, intravenous drug use, or recent invasive procedures presented to the emergency department with a several-day history of fever and rapidly progressive weakness of all four limbs. On admission, the patient was febrile (38.4°C), tachycardic at 110 bpm, with a blood pressure of 110/60 mmHg. Neurological examination revealed symmetric tetraparesis affecting both upper and lower extremities, with a power of 1/5 on the Medical Research Council scale. There was no neck stiffness, photophobia, or loss of consciousness. Cardiac auscultation did not reveal an audible murmur at the time of admission.
The combination of fever and acute tetraparesis prompted initial evaluation for a central nervous system infectious process. Brain magnetic resonance imaging (MRI) at admission demonstrated multiples ischemic lesions. Cerebrospinal fluid (CSF) analysis, obtained by lumbar puncture, revealed mildly elevated protein (0,40 g/L) with a modest pleocytosis [5], without hypoglycorrhachia and with negative Gram stain and culture. Blood cultures were obtained and empirical intravenous antibiotic therapy for suspected bacterial meningitis or meningoencephalitis was initiated with thirs generation cephalosporins.
Failure to Improve and Escalated Investigation
Over the following days, the patient showed no clinically meaningful improvement in his neurological status or fever. Given this lack of response and the ongoing febrile syndrome, repeat brain MRI was performed. The follow-up imaging demonstrated multiple new ischemic lesions distributed across different vascular territories — specifically involving [describe territories, e.g., bilateral hemispheres, cerebellum, brainstem] — a pattern highly suggestive of cardioembolic or septic embolic events rather than a primary central nervous system infection. This finding fundamentally reoriented the diagnostic evaluation toward a cardiac embolic source.
Echocardiographic Assessment
Initial transthoracic echocardiography (TTE), performed upon admission, had not identified any valvular abnormality, vegetation, or perivalvular complication. In light of the new embolic stroke pattern, repeat cardiac imaging was urgently undertaken. A second echocardiographic evaluation revealed extensive structural damage of the aortic valve including complete perforation of a cusp, associated with severe aortic regurgitation on Doppler interrogation. Furthermore, a paravalvular abscess was identified appearing as an echolucent perivalvular cavity (Figures 1–3). These findings established the definitive diagnosis of aortic infective endocarditis with locally uncontrolled infection.
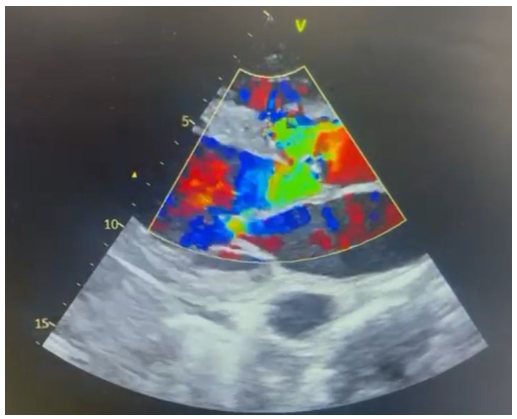
Figure 1. Parasternal long-axis (PLAX) view demonstrating aortic valve perforation and severe aortic regurgitation on color Doppler.

Figure 2. Parasternal long-axis (PLAX) view showing the paravalvular abscess as an echolucent perivalvular cavity adjacent to the aortic annulus.
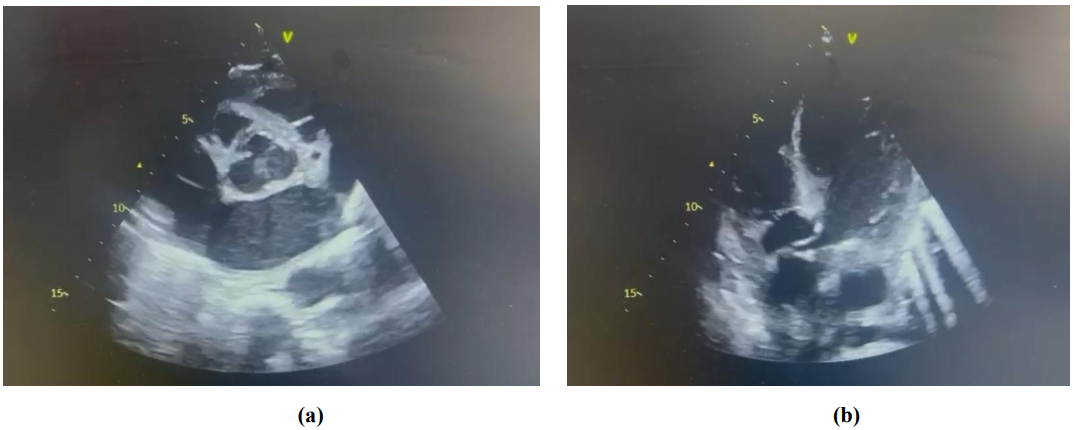
Figure 3. [a] Parasternal short-axis (PSAX) view and [b] Apical five-chamber (A5C) view confirming the paravalvular abscess.
Microbiological Results
Blood cultures obtained at admission were positive Streptococcus spp., Staphylococcus aureus.
Clinical Course and Outcome
Following establishment of the cardiac diagnosis, antibiotic therapy was optimized and a multidisciplinary discussion involving cardiology, cardiac surgery, infectious diseases, and neurology was conducted. Surgical intervention was considered; however, because of the extensive neurological injury, the surgery couldn’t been done. Despite maximal medical management, the patient's clinical condition deteriorated progressively, with worsening hemodynamic instability and neurological decline. The patient died 1 day after admission from complications of advanced IE with severe aortic regurgitation, paravalvular abscess, and multifocal septic cerebral embolism.
Discussion
Neurological Presentations of Infective Endocarditis: Diagnostic Misdirection
The case presented here exemplifies one of the most challenging diagnostic scenarios in internal medicine: a patient with IE whose neurological manifestations entirely dominate the initial clinical picture, masking the underlying cardiac infection. Neurological complications of IE occur in 20–40% of patients with left-sided disease and represent the most frequent extracardiac complication, preceding cardiac diagnosis in a significant minority of cases [5,6]. The spectrum includes ischemic stroke (the most common, occurring in approximately 15–20% of IE cases), transient ischemic attack, symptomatic brain abscess, meningitis, hemorrhagic stroke, and — as in our patient — an acute motor deficit syndrome mimicking infectious myelopathy or meningoencephalitis [4,7].
The pattern of multifocal ischemic infarcts in multiple vascular territories on brain MRI — as observed on the follow-up imaging in our patient — is a critically important diagnostic clue. While a single territorial infarct may reflect atherosclerotic or cardioembolic stroke from conventional sources, the simultaneous or near-simultaneous involvement of multiple arterial territories in a febrile patient should immediately raise suspicion for septic embolism from an intracardiac source [7,11]. Published series report that brain MRI, when performed systematically in IE patients, detects cerebral lesions in up to 80% of cases supporting its routine use early in the diagnostic work-up [12].
The initial misattribution of our patient's presentation to bacterial meningitis was supported by CSF pleocytosis and elevated protein, findings that are well recognized in IE-associated neurological disease and that do not reliably distinguish meningitis from aseptic meningeal reaction to embolic events or subarachnoid micro-hemorrhage [7,13]. This underscores the importance of maintaining IE as an active differential diagnosis even when CSF findings appear compatible with meningitis, particularly in patients who fail to improve on empirical antibiotic therapy.
The Critical Role of Echocardiography in IE Diagnosis — and the Limits of TTE
Echocardiography is the imaging cornerstone of IE diagnosis. The 2023 ESC Guidelines for the Management of Endocarditis recommend TTE as the first-line imaging modality in all patients with suspected IE (Class I), followed by TEE when TTE is negative, non-diagnostic, or technically inadequate, and in any patient with a prosthetic valve or prior IE (Class I) [1]. Critically, the guidelines further recommend repeat TTE or TEE within 5–7 days if clinical suspicion remains high and the initial examination was negative or inconclusive [1].
The diagnostic limitations of TTE for perivalvular complications are well established. In the landmark study by Daniel et al., TTE detected only 28% of perivalvular abscesses confirmed at surgery or autopsy, compared to 87% for TEE [9]. Contemporary data confirm this gap: a 2022 meta-analysis demonstrated that CT had a sensitivity of 88% for abscess detection compared to 74% for TEE, with CT now formally incorporated into the 2023 ESC diagnostic algorithm as a complementary modality alongside echocardiography [10,14]. Valve perforation has a TEE sensitivity of approximately 75% versus only a fraction of that for TTE [10].
In our patient, the initial TTE was unremarkable, which reflects the well-documented insensitivity of this modality for early or subtle perivalvular pathology. The delay between the negative TTE and the eventual diagnosis of valve perforation and paravalvular abscess likely allowed progression of structural destruction to an irreversible degree. This case strongly reinforces the principle articulated in current guidelines: a negative TTE should never be interpreted as exclusion of IE when clinical suspicion — particularly multifocal embolic strokes in a febrile patient — is present [1,8]. TEE and/or cardiac CT should have been performed earlier in the diagnostic pathway.
The 2023 ESC guidelines have expanded the diagnostic toolkit beyond echocardiography to include cardiac computed tomography angiography (CTA) and nuclear imaging (18F-FDG-PET/CT, WBC-SPECT/CT) as complementary modalities, particularly for prosthetic valve IE or when echocardiography is inconclusive [1]. Cardiac CTA, in particular, offers superior sensitivity for perivalvular extension (abscess, pseudoaneurysm) compared to TEE alone, and its combination with echocardiography in cases of suspected complicated IE has been shown to increase overall diagnostic sensitivity to near 100% for abscess detection [10,14].
Paravalvular Abscess and Valve Perforation: High-Risk Features Demanding Urgent Surgery
Paravalvular abscess and valve perforation are among the most severe complications of IE and carry a markedly worsened prognosis compared to uncomplicated disease. Paravalvular abscess occurs in 10–40% of IE cases, with the aortic valve being the most frequently affected site — occurring in approximately 30–40% of aortic valve IE cases [9,15]. It is characterized by the extension of infection beyond the valve annulus into the perivalvular fibrous tissue, creating an echolucent or echodense cavity on echocardiography. Abscess formation is independently associated with higher in-hospital mortality, a higher rate of new conduction disturbances (atrioventricular block, bundle branch block), and an approximately two-fold increase in the need for cardiac surgery compared to IE without abscess [15,16].
Valve perforation results from enzymatic destruction of the leaflet tissue by virulent organisms, leading to acute severe regurgitation and rapid hemodynamic deterioration. In aortic IE, severe aortic regurgitation — whether from leaflet destruction, perforation, or annular dehiscence — produces acute volume overload of the left ventricle, which — unlike in chronic aortic regurgitation — has no compensatory dilation and rapidly progresses to pulmonary edema and cardiogenic shock [16]. The combination of valve perforation and paravalvular abscess, as seen in our patient, represents a particularly advanced and surgically challenging disease state.
The 2023 ESC Guidelines define both of these findings as indications for urgent cardiac surgery (within 3–5 days): aortic or mitral valve IE with evidence of locally uncontrolled infection (abscess, pseudoaneurysm, fistula) is a Class I indication for urgent surgical intervention [1]. Emergency surgery (within 24 hours) is indicated when severe regurgitation causes refractory pulmonary edema or cardiogenic shock [1]. Surgical delay in the setting of uncontrolled local infection allows progressive annular destruction, conduction system involvement, and potentially fatal hemodynamic deterioration — as tragically illustrated in this case.
Neurological Complications and Surgical Decision-Making
The management of cardiac surgery in IE patients with neurological complications is a major clinical dilemma. Concern about hemorrhagic transformation of ischemic lesions under cardiopulmonary bypass anticoagulation has historically led to delays in surgery that may paradoxically worsen outcomes by allowing further valvular destruction and embolism [4,6]. Contemporary evidence and the 2023 ESC guidelines support a more aggressive approach: surgery should not be delayed in patients after transient ischemic attack or after documented non-hemorrhagic ischemic stroke in the setting of heart failure, uncontrolled infection, abscess, or persistent high embolic risk [1]. The risk of hemorrhagic conversion during cardiac surgery is estimated at only 2–7% for ischemic strokes — substantially lower than the risk of recurrent embolism or death from untreated IE complications [1,6].
A significant caveat applies in the presence of large or hemorrhagic cerebral infarction: in patients with significant preoperative hemorrhagic stroke, a delay of at least four weeks is generally recommended before cardiac surgery, given the substantially higher risk of hemorrhagic transformation under anticoagulation [1,6]. In patients with hemorrhagic stroke and unstable hemodynamics, the decision requires careful individualized assessment of the expected neurological outcome versus the cardiac surgical urgency — a dilemma that must be resolved by a multidisciplinary endocarditis team [1].
In our patient, the extent of multifocal cerebral injury and the degree of neurological impairment at the time of cardiac diagnosis were critical factors informing the surgical decision. The delayed recognition of IE had allowed progression to irreversible neurological damage and severe structural valve destruction, and the combination of these factors precluded a beneficial surgical outcome. This highlights how diagnostic delay in neurological-predominant IE directly constrains therapeutic options.
The Endocarditis Team and Multidisciplinary Management
The 2023 ESC guidelines place particular emphasis on the Endocarditis Team as the structural cornerstone of IE management. This team is responsible for real-time decision-making on antibiotic regimens, surgical timing, and complication management [1,17]. Patients with complicated IE, defined by hemodynamic compromise, uncontrolled infection, perivalvular extension, or embolic events, should be managed or consulted in a dedicated Heart Valve Center with immediate surgical facilities [1].
In our case, the delayed assembly of this multidisciplinary framework — a consequence of the initial neurological framing of the presentation — contributed to the delayed cardiac diagnosis and the failure to mobilize a surgical team during the window of potential operability. This underscores the organizational imperative of having pre-established protocols for immediate echocardiographic escalation to TEE in any febrile patient with multifocal embolic strokes, regardless of the initial clinical diagnosis.
Blood Cultures and Microbiological Diagnosis
Blood cultures are the cornerstone of microbiological diagnosis in IE and are positive in approximately 90% of cases when appropriate sampling is performed — ideally three sets from different venipuncture sites before antibiotic initiation [1,8]. In our patient, blood cultures were obtained at admission; however, antibiotic therapy had already been initiated empirically for presumed meningitis, which may have reduced culture yield if sampling occurred after antibiotic administration [1]. This represents a common and preventable source of diagnostic failure: the administration of antibiotics before blood culture collection in febrile patients with neurological presentations delays microbiological identification and complicates antibiotic optimization when IE is subsequently recognized.
When blood cultures remain negative after adequate sampling — a scenario occurring in approximately 10% of IE cases — an expanded etiological workup including serology for Coxiella burnetii, Bartonella spp., Brucella, Tropheryma whipplei, and fungal organisms, as well as broad-range 16S rRNA PCR on valve tissue, should be pursued [1,8]. The causative organism in IE critically influences both antibiotic selection and surgical decision-making: Staphylococcus aureus, for example, is associated with a dramatically higher rate of perivalvular extension, rapid valve destruction, and embolic events compared to oral streptococci, and its identification should prompt immediate surgical evaluation [1,16].
Conclusion
We report a fatal case of aortic infective endocarditis with valve perforation and paravalvular abscess whose diagnosis was critically delayed by the initial neurological framing of the presentation as bacterial meningitis. Three key lessons emerge from this case. First, IE must remain in the differential diagnosis of any febrile patient presenting with acute neurological deficits, particularly when multifocal ischemic strokes in different vascular territories are identified on brain imaging. Second, a negative initial TTE cannot be used to exclude IE, and TEE — or cardiac CT — should be performed promptly when clinical suspicion persists, without waiting for clinical deterioration. Third, the window for potentially curative surgical intervention in IE with perivalvular complications is narrow; diagnostic delay directly forecloses this option. Early systematic cardiac imaging and the immediate activation of a multidisciplinary endocarditis team are the most impactful interventions available to clinicians managing this complex and frequently fatal disease.
References
- Delgado V., Marsan NA., de Waha S., et al. 2023 ESC Guidelines for the management of endocarditis. Eur Heart J. 2023;44(39):3948–4042. [PubMed.]
- Murdoch DR., Corey GR., Hoen B., et al. Clinical presentation, etiology, and outcome of infective endocarditis in the 21st century: the International Collaboration on Endocarditis-Prospective Cohort Study. Arch Intern Med. 2009;169(5):463–473. [PubMed.]
- Cahill TJ., Baddour LM., Habib G., et al. Challenges in infective endocarditis. J Am Coll Cardiol. 2017;69(3):325–344. [PubMed.]
- Thuny F., Avierinos JF., Tribouilloy C., et al. Impact of cerebrovascular complications on mortality and neurologic outcome during infective endocarditis: a prospective multicentre study. Eur Heart J. 2007;28(9):1155–1161. [PubMed.]
- García-Cabrera E., Fernández-Hidalgo N., Almirante B., et al. Neurological complications of infective endocarditis: risk factors, outcome, and impact of cardiac surgery. Circulation. 2013;127(23):2272–2284. [PubMed.]
- Okazaki S., Yoshioka D., Sakaguchi M., et al. Acute ischemic brain lesions in infective endocarditis: incidence, related factors, and postoperative outcomes. Cerebrovasc Dis. 2013;35(2):155–162. [PubMed.]
- Sonneville R., Mirabel M., Hajage D., et al. Neurologic complications and outcomes of infective endocarditis in critically ill patients: the Endocardite En Reanimation prospective multicenter study. Crit Care Med. 2011;39(6):1474–1481. [PubMed.]
- Nishimura RA., Otto CM., Bonow RO., et al. 2014 AHA/ACC Guideline for the Management of Patients with Valvular Heart Disease. J Am Coll Cardiol. 2014;63(22):e57–185. [PubMed.]
- Daniel WG., Mugge A., Martin RP., et al. Improvement in the diagnosis of abscesses associated with endocarditis by transesophageal echocardiography. N Engl J Med. 1991;324(12):795–800. [PubMed.]
- Fagman E., Perrotta S., Bech-Hanssen O., et al. ECG-gated computed tomography: a new role for patients with suspected aortic prosthetic valve endocarditis. Eur Radiol. 2012;22(11):2407–2414. [PubMed.]
- Klein I., Iung B., Labreuche J., et al. Cerebral microbleeds are frequent in infective endocarditis: a case-control study. Stroke. 2009;40(9):3202–3207. [PubMed.]
- Duval X., Iung B., Klein I., et al. Effect of early cerebral magnetic resonance imaging on clinical decisions in infective endocarditis: a prospective study. Ann Intern Med. 2010;152(8):497–504. [PubMed.]
- Ruttmann E., Willeit J., Ulmer H., et al. Neurological outcome of septic cardioembolic stroke after infective endocarditis. Stroke. 2006;37(8):2094–2099. [PubMed.]
- Habets J., Tanis W., Reitsma JB., et al. Comparing the diagnostic accuracy of computed tomography versus transoesophageal echocardiography for infective endocarditis: a systematic review and meta-analysis. Eur Radiol. 2022;32(7):4752–4762. [PubMed.]
- Anguera I., Miro JM., Vilacosta I., et al. Aorto-cavitary fistulous tract formation in infective endocarditis: clinical and echocardiographic features of 76 cases and risk factors for mortality. Eur Heart J. 2005;26(3):288–297. [PubMed.]
- Moreillon P., Que YA. Infective endocarditis. Lancet. 2004;363(9403):139–149. [PubMed.]
- Mestres CA., Paré JC., Miró JM; Working Group on Infective Endocarditis of the Hospital Clínic de Barcelona. Organization and functioning of a multidisciplinary team for the diagnosis and treatment of infective endocarditis: a 30-year perspective (1985-2014). Rev Esp Cardiol. 2015;68(5):363–368. [PubMed.]