>Corresponding Author : Z El Jaouhari
>Article Type : Case Report
>Volume : 6 | Issue : 2
>Received Date : 23 Feb, 2026
>Accepted Date : 06 March, 2026
>Published Date : 20 March, 2026
>DOI : https://doi.org/10.54289/JCRMH2600107
>Citation : El Jaouhari Z, Megzari M, Belmalyani R, Bouziane M, Haboub M, et al. (2026) Hyperthyroidism and Atrioventricular Block: A Case Report. J Case Rep Med Hist 6(2): doi https://doi.org/10.54289/JCRMH2600107
>Copyright : © 2026 El Jaouhari Z, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Case Report | Open Access | Full Text
Cardiology department, Chu Ibn Rochd Casablanca, Morocco
*Corresponding author: Zineb El jaouhari, Cardiology department, Chu Ibn Rochd Casablanca, Morocco
Introduction
The cardiac conduction system is essential for maintaining a coordinated heart rhythm. It begins in the sinus node (or sinoatrial node), located in the right atrium, which generates the electrical impulse. This impulse spreads through the atria, then reaches the AV node, which acts as a relay. The AV node slows the impulse before it travels to the ventricles via the bundle of His and the Purkinje fibers. When a blockage occurs at any level of this pathway, an atrioventricular block (AVB) may occur.
Thyroid hormones play an essential role in maintaining normal cardiac function, particularly by modulating heart rate, myocardial contractility, and electrical conduction. In hypothyroidism, decreased thyroid hormone levels may lead to bradycardia, prolongation of the PR and QT intervals on the electrocardiogram (ECG), and in some cases more severe conduction disturbances such as AVB.
In contrast, the mechanisms underlying the effects of hyperthyroidism on the cardiac conduction system are not clearly established. Conduction disturbances related to hyperthyroidism remain rare (5–10%). They are mainly represented by atrioventricular blocks (AVB), the most frequent being first-degree AVB.
In this context, we report a case of hyperthyroidism revealed by a high-degree AVB.
Case Report
We report the case of a 62-year-old woman with hypertension treated with Medzar 50 mg once daily, with no other significant medical history, who presented to the emergency department for dizziness without episodes of syncope.
Clinical examination revealed a blood pressure of 150/90 mmHg and bradycardia with a heart rate of 33 beats per minute, along with the presence of a retrosternal goiter on neck examination. The remainder of the physical examination was unremarkable. The electrocardiogram (ECG) showed a high-degree 2:1 AVB with a junctional escape rhythm at 33 beats per minute.
Transthoracic echocardiography was performed and showed no structural cardiac abnormalities, with a left ventricular ejection fraction (LVEF) of 60%.
Laboratory investigations revealed a decreased TSH level of 0.31 mIU/L, with elevated free thyroid hormones: free T3 at 5.5 ng/dL and free T4 at 1.7 ng/dL. No other biological abnormalities were detected, particularly no anemia, no electrolyte disturbances, and no elevated inflammatory markers.
Cervical ultrasound demonstrated a heterogeneous multinodular goiter, with the most suspicious nodule classified as EU-TIRADS 4.
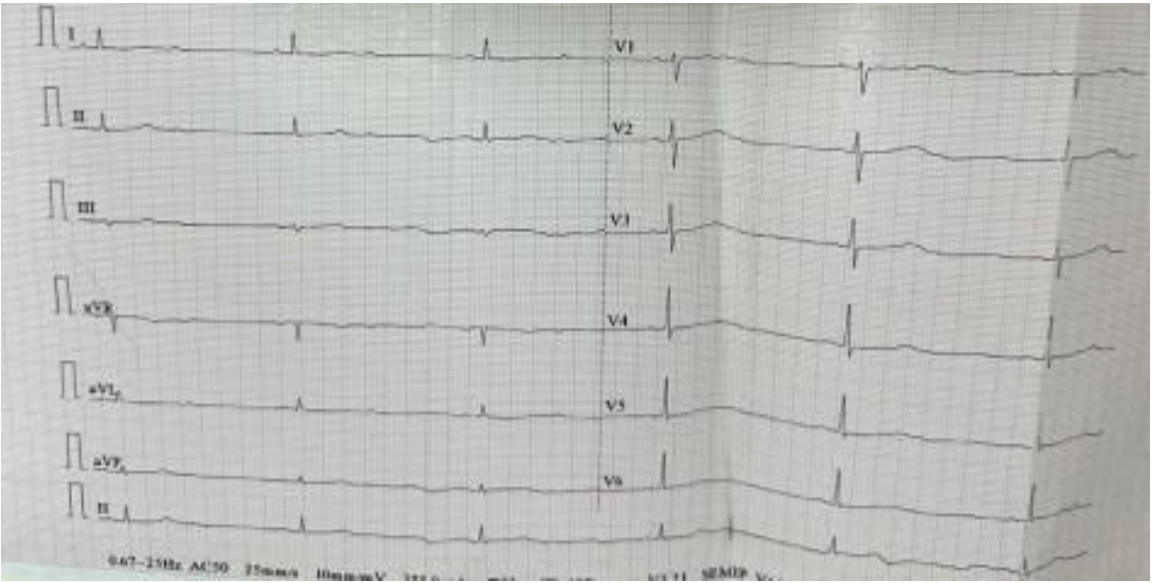
Figure 1. ECG showing high-degree 2:1 atrioventricular block with an escape rhythm at 33 bpm
A 24-hour ECG Holter monitoring showed sinus rhythm with frequent paroxysmal episodes of high-degree atrioventricular block.
Consequently, treatment with Methimazole (Dimazole) 10 mg/day was initiated. Daily ECG monitoring showed no recurrence of high-degree AVB following initiation of antithyroid treatment.
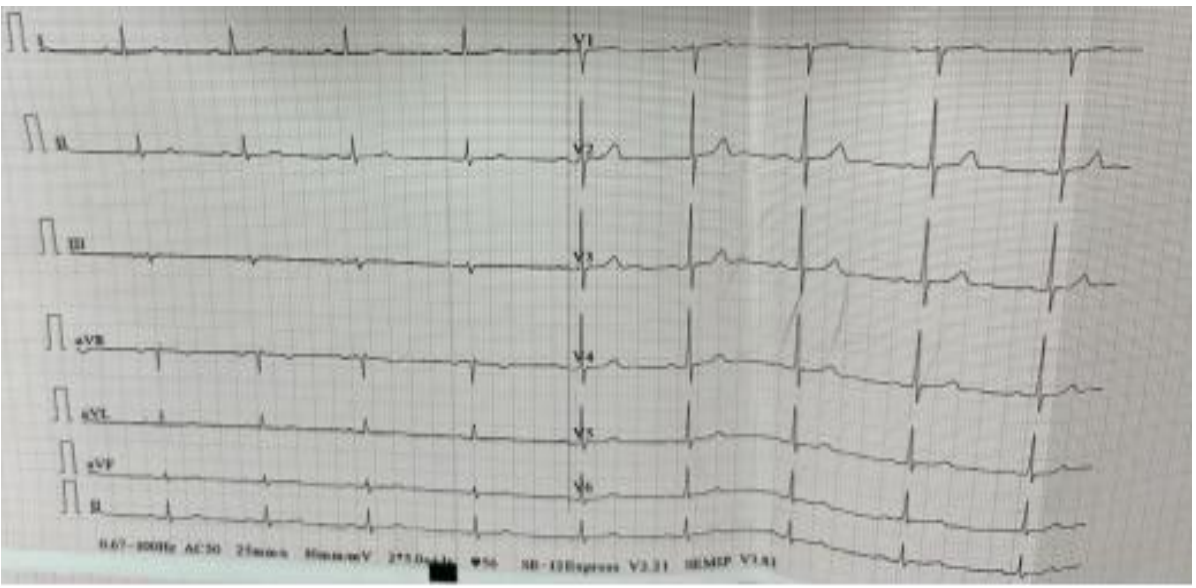
Figure 2. ECG after initiation of antithyroid drug therapy
A 48-hour ECG Holter performed on day 7 of treatment showed sinus rhythm without any episodes of atrioventricular block of any degree. Thyroid function tests had normalized, with TSH at 0.5 mIU/L and free T3 at 4 ng/L.
Therefore, the diagnosis of thyrotoxic induced atrioventricular block secondary to hyperthyroidism was established, and the patient was discharged with close follow-up.
Discussion
Hyperthyroidism most commonly leads to supraventricular or ventricular arrhythmias.
Atrioventricular blocks related to hyperthyroidism are very rare, and their mechanisms remain poorly understood. A review of the literature identified seven documented cases: five cases of high-degree AVB, one case of first-degree AVB, and one case of sinus bradycardia [1].
A similar observation to ours was published at the CHU IBN ROCHD in 2020 [2], describing a paroxysmal high-degree AVB associated with hyperthyroidism that regressed after initiation of antithyroid drug therapy.
A comparable case was reported in 1987 by Archambeaud-Mouveraux [3]. The patient had severe hyperthyroidism and presented with alternating second- and third-degree AVB over a six-year period. Hyperthyroidism was eventually diagnosed, and the conduction abnormalities completely resolved after restoration of euthyroidism.
Toloune F [4] also reported the case of a young patient with Graves’ disease who presented on ECG with first-degree AVB and Mobitz type I second-degree AVB. These conduction abnormalities likewise disappeared after return to euthyroid status. Three other studies described similar findings.
Topaloglu S [5], in Turkey, described two cases of hyperthyroidism with complete AVB that permanently resolved after treatment of the thyroid disease. Atri et al. [6], in India, also reported a case of second-degree AVB due to hyperthyroidism that fully regressed under antithyroid drug therapy.
As early as 1980, Miller RH [7] compiled 35 cases of AVB secondary to hyperthyroidism, all of which were reversible with antithyroid treatment. These cases were investigated using intracardiac electrophysiological studies and were found to be nodal in origin.
It should be noted that most reported cases involved Graves’ disease. This led some authors to suggest a possible immunological mechanism, such as autoimmune myocarditis associated with Graves’ disease. However, this hypothesis was not confirmed, as no evidence of myocarditis was identified in these cases.
In reality, hyperthyroidism is more commonly responsible for supraventricular rhythm disorders (reported in 2–20% of cases depending on the series), and less frequently for ventricular arrhythmias. Another mechanism has been suggested, though not confirmed: hyperstimulation of the atrioventricular node leading to a reflex mechanism of increased vagal tone. In fact, the mechanisms underlying conduction abnormalities in hyperthyroidism remain poorly understood.
The occurrence of a conduction disorder during hyperthyroidism may also be coincidental. Indeed, in most reported cases, infectious or iatrogenic factors were present and could independently explain the development of atrioventricular block (AVB). The rapid regression of the conduction disorder further supports this hypothesis. In other cases, underlying valvular, ischemic, or degenerative heart disease was identified.
Congenital block is more difficult to assess and accounts for approximately 3–5% of AVB cases, particularly in the absence of prior ECG recordings. Persistence of the conduction abnormality after correction of thyroid dysfunction would favor this etiology.
Cases in which hyperthyroidism alone appears to be responsible for conduction disturbances are exceptional. When this occurs, no other predisposing condition explains the AVB, and normalization of atrioventricular conduction occurs in parallel with restoration of euthyroidism.
In our case, no clinical, structural, or biological abnormality other than hyperthyroidism could explain the occurrence of the AVB. Its regression following antithyroid therapy, along with normalization of thyroid function tests, strengthens the hypothesis of a causal relationship.
Conclusion
Exceptionally, hyperthyroidism alone may be responsible for complete atrioventricular block. Possible mechanisms underlying these conduction disturbances include thyrotoxic myocarditis and/or autoimmune processes.
The present case highlights the importance of considering hyperthyroidism as a contributory factor in the development of atrioventricular block. It also underscores the need for thorough clinical and biological evaluation in patients presenting with unexplained cardiac symptoms. Treatment of hyperthyroidism led to significant improvement of the conduction disorder, supporting the concept that appropriate management of thyroid dysfunction can directly influence the resolution or attenuation of cardiac conduction abnormalities.
This report emphasizes the importance of a comprehensive diagnostic approach to any cardiac conduction disorder.
References
- Moustaghfir A., Kharchafi A., Mahassin F., Chaari J., Ghafir D., et al. Dysfonction sinusale au cours d’une maladie de Basedow. A propos d’une observation. Rev Médecine Interne. 1999;20(9):804–5. [Ref.]
- Mahoungou–Mackonia N., Baragé., Nouamou I., Arous S., Bennouna G., et al. Bloc auriculoventriculaire de haut degré révélant une Maladie de Basedow: A propos d’un cas, Service de cardiologie, chu–ibn ROCHD, Casablanca. Maroc 3. [PubMed.]
- Archambeaud–Mouveroux F., Roussanne A., Jadaud J., Dejax C., Blanc P., et al. Prolonged hyperthyroidism and recurrent atrio–ventricular block. Rev Med Interne. 1987;8(2):213–7. [PubMed.]
- Toloune F., Boukili A., Ghafir D., Hadri L., Chaari J., et al. Hyperthyroïdism with atrioventricular block: a pathogenetic hypothesis, à case report with review. Arch Mal Coeur Vaiss. 1988;81(9):1131–5. [PubMed.]
- Topaloglu S., Topaloglu OY., Ozdemir O., Soylu M., Demir AD., et al. Hyperthyroidism and complete atrioventricular block––a report of 2 cases with electrophysiologic assessment. Angiology. 2005;56(2):217–20. [PubMed.]
- Atri SK., Chugh SN., Goya S., Chugh K. Reversible atrioventricular blocks in thyroid storm. J Assoc Physicians India. 2011;59:178–9. [PubMed.]
- Miller RH., Corcoran FH., Baker WP. Second and third degree atrioventricular block with Graves’ disease: a case report and review of the literature. Pacing Clin Electrophysiol. 1980;3(6):702–11. [PubMed.]