>Corresponding Author : Hlaibi Omnia
>Article Type : Case Report
>Volume : 6 | Issue : 1
>Received Date : 25 Jan, 2026
>Accepted Date : 06 Feb, 2026
>Published Date : 11 Feb, 2026
>DOI : https://doi.org/10.54289/JCRMH2600105
>Citation : Hasnae S, Omnia H, Amina G, Boufettal H, Mahdaoui S, et al. (2026) Incidental Discovery of Endometrial Cancer: A Case Report. J Case Rep Med Hist 6(1): doi https://doi.org/10.54289/JCRMH2600105
>Copyright : © 2026 Hasnae S, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Case Report | Open Access | Full Text
1Departement of gynecology and obstetrics, University Hospital Center Ibn Rochd, Casablanca 20100, Morocco
2Faculty of Medicine and Pharmacy, Hassan II University of Casablanca, Casablanca, Morocco
*Corresponding author: Hlaibi Omnia, Departement of gynecology and obstetrics, University Hospital Center Ibn Rochd, Casablanca 20100, Morocco and Faculty of Medicine and Pharmacy,Hassan II University of Casablanca,Casablanca, Morocco
Abstract
Background: Endometrial cancer is rarely discovered incidentally during surgical management of a presumed benign condition. Observation: A 75-year-old postmenopausal patient presented with a large adnexal mass associated with an incidental finding of grade 1 endometrioid adenocarcinoma, limited to the endometrium.
Discussion: This case illustrates the importance of comprehensive management by total hysterectomy with bilateral adnexectomy in postmenopausal women with giant adnexal masses, enabling the diagnosis and treatment of concomitant endometrial lesions.
This case illustrates the importance of comprehensive management by total hysterectomy
Conclusion: The application of international recommendations ensures appropriate staging and therapeutic management.
Keywords: Endometrial Cancer, Incidental Finding, Mucinous Cystadenoma, Endometrioid Adenocarcinoma, Gynaecological Surgery
Introduction
Endometrial cancer is the most common gynaecological malignancy in industrialised countries, occurring mainly after menopause [1]. It is typically revealed by post-menopausal metrorrhagia, but incidental diagnoses during pelvic surgery for presumed benign pathology remain possible, although rare [2,3]. The association with a large benign adnexal tumour, such as a mucinous ovarian cystadenoma, complicates the clinical and radiological picture and may suggest anovarian malignancy [4,5].
Clinical case
Clinical presentation
A 75-year-old female patient, single, nulliparous, menopausal for 20 years, consulted for chronic pelvic pain developing over 5 months, associated with significant progressive abdominal distension without other gynaecological, digestive or urinary signs. Clinical examination revealed an abdominal-pelvic mass measuring approximately 30 cm, with the upper limit at the xiphoid process, generally cystic in consistency, Figure 1, with no tenderness or palpable mass elsewhere; the rest of the physical examination was unremarkable.

Figure 1. Clinical image of abdominal distension
Radiological investigations
The abdominal-pelvic CT scan reveals a large cystic massin the abdomen and pelvis containing fluid, with a thin wall, partitioned, without vegetation orisolated solid components, measuring 32 × 26 × 18 cm, consistent with a benign adnexal tumour Figure 2.
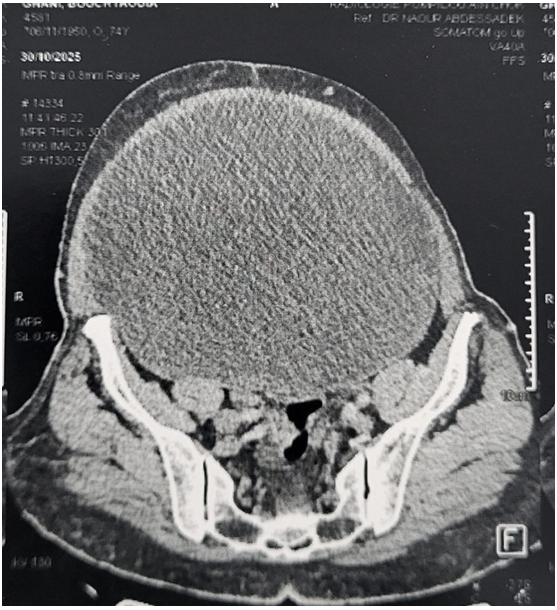
Figure 2. CT scan image of the abdominal mass
Surgical exploration and histology
A median laparotomy was performed, revealing an adnexal mass measuring 36 × 27 × 26 cm, with no signs of peritoneal carcinomatosis or macroscopic ascites, and a moderately enlarged uterus. The surgical procedure consisted of a total hysterectomy with bilateral adnexectomy, multiple peritoneal biopsies, omentum biopsy and collection of peritoneal lavage fluid.
The pathological examination concluded that there was endometrioid adenocarcinoma of the endometrium, grade 1 (Fuhrman score), limited to the endometrium without myometrial invasion, associated with a benign ovarian mucinous cystadenoma. The peritoneal and omental biopsies and peritoneal lavage were free of malignancy, notably the absence of peritoneal carcinomatosis.
Discussion
Diagnostic and epidemiological characteristics
The diagnosis of endometrial cancer is usually considered in cases of post-menopausal metrorrhagia, which was not the case in this patient, making the discovery of the tumour strictly incidental on the hysterectomy specimen. The incidence of gynaecological cancers discovered unexpectedly in surgical specimens after surgery for presumed benign pathology remains low, estimated at 2-5% depending on the series, but is well documented in the literature [2,3].
Large adnexal masses, particularly mucinous cystadenomas, frequently manifest as progressive abdominal distension and pelvic pain, without specific signs of malignancy. Imaging (ultrasound, CT scan, MRI) allows partial characterisation of the lesion, but the formal distinction between benign and malignant ovarian tumours, as well as the detection of concomitant endometrial neoplasia, is based on definitive histological examination [6].
Histological and prognostic characteristics
Grade 1 endometrioid adenocarcinoma limited to the endometrium corresponds to a very early stage (stage 1a, according to the FIGO 2009 classification) with an excellent prognosis when complete surgical treatment is performed. The ESGO/ESTRO/ESP (2025) and consider this type of tumour, in the absence of myometrial invasion and associated risk factors, to be a very low-risk group that does not warrant systematic adjuvant treatment [1,7]. Ovarian mucinous cystadenoma is a benign epithelial tumour derived from the coelomic epithelium, capable of reaching large sizes, sometimes exceeding 30 cm, as described in numerous cases of ‘giant mucinous cystadenoma’ [4,5]. The absence of solid components, intracavitary vegetations, thickened walls and peritoneal carcinomatosis, combined with benign histology, confirms the non-malignant nature of the adnexal tumour in this case. The malignant risk of a mucinous cystadenoma is less than 1% in the absence of suspicious features on imaging and surgery [5].
Therapeutic strategy and staging in postmenopausal patients with a large adnexal mass, total hysterectomy with bilateral adnexectomy is often recommended, allowing both treatment of the mass and diagnosis of any concomitant endometrial lesions [1,6]. In the reported case, hysterectomy combined with peritoneal biopsies and peritoneal lavage enabled complete staging and curative treatment of the incidental endometrial cancer. According to the ESGO/ESTRO/ESP risk criteria (2025), this patient has very low-risk endometrial cancer, justifying surveillance alone without adjuvant treatment (chemotherapy or radiotherapy). Surveillance includes regular clinical examination every 3-4 months in the first year, then every 6 months for 5 years, supplemented if necessary by pelvic imaging (ultrasound or MRI) [1,7].
Conclusion
This case illustrates the possibility of incidental discovery of low-grade endometrial cancer at a very early stage during surgical management of a large, apparently benign adnexal tumour. Total hysterectomy with bilateral adnexectomy in postmenopausal women with a giant adnexal mass not only allows Total hysterectomy with bilateral adnexectomy in postmenopausal women with a giant adnexal mass not only allows for the treatment of the ovarian tumour but also the diagnosis and treatment of associated endometrial lesions, with a major prognostic impact. Rigorous application of international recommendations (ESGO/ESTRO/ESP, NCCN) for the staging and treatment of endometrial cancer ensures management tailored to the risk profile and avoids unnecessary adjuvant treatments in patients at very low risk. This case highlights the importance of complete histological examination of all intraoperative samples, a cornerstone of modern gynaecological oncology.
References
- Colombo N., Creutzberg C., Amant F., et al. Management of Patients Diagnosed with Endometrial Cancer: ESGO‒ESTRO‒ESP guidelines update. Cancers (Basel). 2023;15(3):765. [Ref.]
- Ekici MA., Ozer A., Akgün N., et al. Likelihood of incidental finding of gynecological cancer in hysterectomy specimens for presumed benign disease. Eur J Gynaecol Oncol. 2020;41(3):433‒438. [Ref.]
- Ouldamer L., Caille A., Barranger E., et al. Risk of incidental finding of endometrial cancer at the time of hysterectomy for benign indications. J Minim Invasive Gynecol. 2014;21(3):509‒515. [PubMed.]
- Acién P., Quereda F., García-García E. A huge mucinous cystadenoma of ovarian: a rare case report. Case Rep Obstet Gynecol. 2014;6(2):5225. [PubMed.]
- International Journal of Reproductive Medicine. Mixed benign Brenner tumor with mucinous cystadenoma of the ovary in a postmenopausal woman: case report and review. Int J Womens Health. 2024;16:1285‒1298. [Ref.]
- Patel MD., Ascher SM., Paspulse B., et al. Management of Incidental Adnexal Findings on Computed Tomography and Magnetic Resonance Imaging. J Am Coll Radiol. 2020;17(2):248‒254. [PubMed.]
- Concin N., Matias-Guiu X., Vergote I., et al. ESGO/ESTRO/ESP guidelines for the management of patients with endometrial carcinoma. Int J Gynecol Cancer. 2021;31(1):12‒39. [PubMed.]