>Corresponding Author : Hlaibi Omnia
>Article Type : Case Report
>Volume : 6 | Issue : 1
>Received Date : 30 Dec, 2025
>Accepted Date : 12 Jan, 2026
>Published Date : 24 Jan, 2026
>DOI : https://doi.org/10.54289/JCRMH2600102
>Citation : Omnia H, Hasnae S, Intissar S, Boufetta H, and Mahdaoui S, et al. (2026) Parietal Mass Revealing Parietal Endometriosis: About Two Cases. J Case Rep Med Hist 6(1): doi https://doi.org/10.54289/JCRMH2600102
>Copyright : © 2026 Omnia H, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Case Report | Open Access | Full Text
1Department of Gynecology and Obstetrics, University Hospital Center Ibn Rochd, Casablanca 20100, Morocco
2Faculty of Medicine and Pharmacy, Hassan II University of Casablanca, Casablanca, Morocco
*Corresponding author: Hlaibi Omnia, Department of Gynecology and Obstetrics, University Hospital Center Ibn Rochd, Casablanca 20100, Morocco and Faculty of Medicine and Pharmacy, Hassan II University of Casablanca, Casablanca, Morocco authors
Abstract
Abdominal wall scar endometriosis is a rare entity. It most often occurs on a caesarean section scar in a woman who is genitally active. Its pathophysiology remains unclear, and the most widely accepted hypothesis seems to be in situ cellular grafting during opening of the musculoaponeurotic spaces after hysterotomy. The association of a more or less algic scar mass with cyclic pain is suggestive of the diagnosis. Confirmation can only be histological, and the best treatment is surgical with wide excision. We report two cases of parietal endometriosis on caesarean section scars. The diagnosis was strongly suggested by clinical examination and confirmed by pathological examination. Wide excision of the parietal lesion resulted in recovery without recurrence.
Keywords: Parietal Endometriosis, Pelvic MRI, Cyclic Parietal Pain
Introduction
Endometriosis affects 8-15% of genitally active women. It is defined by the existence of endometrial tissue outside the uterine cavity. The endopelvic form of this pathology is the most common. But it can affect almost any organ except the spleen. The most frequent extrapelvic locations include the lung, gallbladder, small intestine and colon, kidneys, rectovaginal septum, and abdominal wall (rectus sheath, inguinal and umbilical hernias). This pathology is also found on abdominopelvic scars: episiotomies, uterine surgery scars, caesarean section scars, the path of an amniocentesis needle and trocar orifice, and more rarely on appendectomy scars [1].
Parietal endometriosis is rare. It occurs in 1 to 4% of cases of extragenital endometriosis, and its incidence after caesarean section varies from 0.03 to 0.4% [2].
Observation
Thirty-eight-year-old patient, with two live children by caesarean section, consulting for Dysmenorrhoea and cyclic pelvic pain evolving for 6 months with, on clinical examination, an indurated mass measuring 4x3 cm opposite the external right side of the pfannestiel scar, pelvic ultrasound objectifying a deep, finely hypoechoic parietal nodular formation, measuring 32.7 x 12.7 mm, communicating with the pelvic cavity through a 4-mm diameter opening, suggesting an endometriotic nodule, followed on pelvic CT and MRI by a 35x20-mm nodular tissue mass of the rectus abdominis, suggesting parietal endometriosis (figure 1) associated with minimal subperitoneal endometriosis.
Surgical treatment consisted of resection of the endometriotic nodule, with pathological examination revealing fibrofatty and muscular tissue at the site of endometrial mucosal islands. The glands were cystized in places and lined with pseudostratified columnar cells free of cytonuclear atypia in favor of endometriosis.
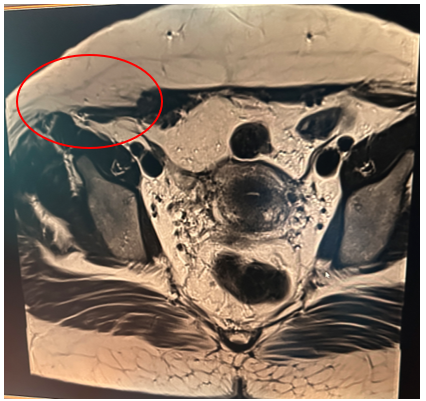
Figure 1.
Observation 2
44-year-old patient with three live children by caesarean section with median incision under the umbilicus, consulted for a painful umbilical nodular swelling with petechiae and cyclic bleeding (figure 2).
Abdomino-pelvic CT scan showed an incisional supra-umbilical hernia with epiploic and uncomplicated digestive content, while pelvic MRI revealed soft-tissue nodules above and below the umbilicus, raising the initial suspicion of a parietal endometrioma (figures 3,4).
The surgical procedure involved resection of the mass (figure 5), with pathological examination revealing a polypoid congestive lesion with a congestive, lobulated surface, the site of haemorrhagic and fibrous remodelling, and comprising regularly lined endometrial glandular structures with no cytonuclear atypia, surrounded by a cytogenic stroma with no signs of malignancy, all in favour of parietal cutaneous endometriosis with no signs of malignancy.
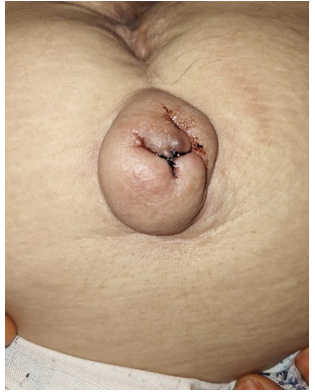
Figure 2. Painful umbilical nodular swelling with petechiae and cyclical bleeding
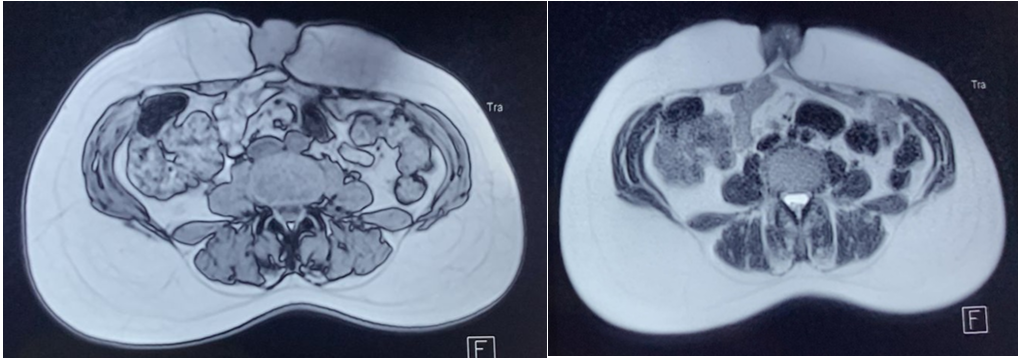
Figure 3-4: Soft tissue nodules above and below the umbilicus

Figure 5: Wide excision of the umbilical mass
Discussion
The term parietal endometrioma is used to designate a mass-forming pelvic or extra-pelvic endometriosis [1].
Parietal endometriosis is rare. It accounts for 1 to 4% of cases of extragenital endometriosis. Very rarely primary, it generally occurs on scars from gynaecological or obstetric surgery, notably episiotomies, uterine surgery scars, caesarean section scars, the path of an amniocentesis needle or a laparoscopic trocar orifice. Its incidence after caesarean section varies from 0.03 to 0.4%, depending on the study [2].
Umbilical or inguinal lesions are also difficult to diagnose, as they may mimic hernial pathology. These lesions appear on average 2.3 years (more often than 90% of cases) after Caesarean section [3].
For parietal endometriomas, the most likely mechanism is local grafting of endometrial cells, which develop in a specific context. Endometrial cells have a high potential for development in non-epithelialized areas. Their development is also favored by secondary inflammation induced by immunological factors. The metaplastic theory has also been proposed to explain parietal endometriomas. Endometrioma arises from multipotential primitive mesenchymal cells that undergo specific metaplastic differentiation [4].
Clinically, it takes the form of an abdominal parietal mass at the level of the caesarean section scar, which may be responsible for cyclical pain [5]. The cyclical nature of the pain is an important element of orientation, but it is far from essential for evoking the diagnosis. Finally, when the lesion is very superficial, a cyclical change in color may be observed, turning bluish and even fistulating to the skin in the form of a bloody discharge. Palpation of the lesion should enable its size and deep location to be appreciated, as the lesion frequently invades the abdominal muscles and their sheaths [1].
On imaging, it is most often located within the cutaneous and subcutaneous planes, more rarely within the muscular plane. On ultrasound, performed with a high-frequency linear probe, it appears as a heterogeneous, round or oval parietal mass, usually solid and hypoechoic, with small cystic portions associated with recent haemorrhage, sometimes vascularized on Doppler (the larger the lesion and the more irregular the boundaries), associated with hyperechoic fat around the perimeter, testifying to contiguous inflammation [5].
Due to its specificity and sensitivity, MRI is the examination of choice for diagnosing endopelvic, extra-pelvic and parietal endometriosis. Signal abnormalities include heterogeneous foci of T1 and/or T2 hyper-signal with fat saturation in the endometrioid nodule, corresponding to the aged, spawned blood accumulated during menstruation. Tissue fibrosis and inflammation around the nodule give a T1 and T2 spin echo signal similar to that of muscle, with or without gadolinium enhancement [6].
The treatment for these lesions is total surgical excision. Exeresis must be wide, involving the entire lesion and extending at least 5 mm into the healthy zone. Parietal reconstruction after exeresis sometimes requires the insertion of a parietal prosthesis when closure of the musculoaponeurotic margins is impossible [7].
The preventive treatment of parietal endometriomas is therefore the quality of surgical closure of the uterus during caesarean sections, and pressure washing of the operative scar margins prior to closure with a saline solution [8].
Conclusion
Parietal endometriosis is rare, and generally occurs on scars from gynaecological or obstetric surgery.
Clinically, it presents as an abdominal parietal mass at the level of the parietal scar. The cyclical nature of the pain is an important, but not indispensable, element of diagnostic orientation.
Thanks to its specificity and sensitivity, MRI is the examination of choice for diagnosing endometriosis.
The treatment of these lesions is wide surgical excision.
Prevention lies in the quality of surgical closure of the uterus during surgery.
References
- Picod G., Boulanger L., Bounoua F., Leduc F., & Duval G. Endométriose pariétale sur cicatrice de césarienne: à propos de 15 cas. Gynécologie Obstétrique & Fertilité. 2006;34(1):8–13. [PubMed.]
- Khlifi A., Kouira M., Anis M., Sonia Z., Ines L. Endométriose pariétale sur cicatrice de césarienne: à propos de 3 cas. Imagerie de La Femme. 2012;22(3):156–161. [PubMed.]
- Merlot B., Ploteau S., Abergel A., Rubob C., Hocke C., et al. Endométriose extra-génitale: atteinte pariétales, thoraciques, diaphragmatiques et nerveuses. RPC Endométriose CNGOF-HAS. Gynécologie Obstétrique Fertilité & Sénologie. 2018;46(3):319–325. [PubMed.]
- Boufettal H., Hermas S., Boufettal R., Jai SR., Kamri Z., et al. Endométriose de cicatrice de la paroi abdominale. La Presse Médicale. 2009;38(1):e1–e6. [Ref.]
- Delebecq J., Duraes M., Mandoul C., Rathat G., Taourel P., et al. Complications postopératoires du quotidien en gynécologie et obstétrique. Imagerie de La Femme. 2020;1–12. [PubMed.]
- Darouichi M. Endométriose ombilicale primitive et secondaire. Feuillets de Radiologie. 2013;53(1):21–26. [Ref.]
- Hafidi R., Kouach J., Yakka M., Salek G., Oukabli M., et al. L’endométriose cicatricielle de la paroi abdominale. Imagerie de La Femme. 2011;21(3):125–127. [Ref.]
- Durand X., Daligand H., Aubert P., Baranger B. Endométriose de la paroi abdominale. Journal de Chirurgie Viscérale. 2010;147(5):354–359. [Ref.]