>Corresponding Author : Benhaddouga Khadija
>Article Type : Case Report
>Volume : 5 | Issue : 8
>Received Date : 06 July, 2025
>Accepted Date : 16 July, 2025
>Published Date : 20 July, 2025
>DOI : https://doi.org/10.54289/JCRMH2500136
>Citation : Moustatir M, Benhaddouga K, Mazhour M, Chyate FZ, Benchrefi Y, et al. (2025) Papillary Adenocarcinoma of the Vagina and Rectum: 1 Case Report and Review of the Literature. J Case Rep Med Hist 5(8): doi https://doi.org/10.54289/JCRMH2500136
>Copyright : © 2025 Moustatir M, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Case Report | Open Access | Full Text
1Resident Physician, Department of Gynecology and Obstetrics, at Ibno Rochd University Hospital, Casablanca, Morocco
2Professor in the Department of Gynecology and Obstetrics at the Ibno Rochd University Hospital in Casablanca, Morocco
*Corresponding author: Benhaddouga Khadija, Resident Physician, Department of Gynecology and Obstetrics, at Ibno Rochd University Hospital, Casablanca, Morocco
Abstract
Papillary adenocarcinoma of the vagina is an extremely rare entity, often associated with hormonal exposure or congenital anomalies. Its coexistence with papillary adenocarcinoma of the rectum is exceptional and raises questions as to whether they are of common or metastatic origin. We present here a review of current knowledge on these rare forms of cancer, with a discussion of differential diagnosis, management and prognosis.
Keywords: Papillary adenocarcinoma, Vagina, Rectum, Synchronous tumors, Rare gynecological cancer
Abbreviations: DES: Diethylstilbestrol, CT: Computed Tomography, ADK: Adenocarcinoma, CK7: Cytokeratin 7, CK20: Cytokeratin 20, CDX2: Caudal Type Homeobox 2, PAX8: Paired Box Gene 8, MRI: Magnetic Resonance Imaging
Introduction
Papillary adenocarcinoma of the vagina is an uncommon malignancy, accounting for less than 1% of all gynaecological cancers. When it occurs outside the context of diethylstilbestrol (DES) exposure, it is considered particularly unusual [1]. The vaginal mucosa is usually the site of squamous cell carcinomas, which makes glandular tumours all the rarer. Papillary adenocarcinoma of the rectum is an infrequent histological form of colorectal cancer, often confused with other subtypes due to its morphological characteristics [2]. The concomitant occurrence of these two entities in the same patient raises complex diagnostic, therapeutic and prognostic issues.
Case Report:
This is a 39-year-old genitally active patient, operated on 2 times in 2015 and 2018 for endometriotic cyst (undocumented), presenting for further management of an invasive papillary adenocarcinoma of the vagina and rectum.
Her history of the disease dates back 2? years, with chronic pelvic pain, profound dyspareunia, urinary signs such as acute urinary retention on several occasions, and digestive signs such as chronic constipation. All this evolving in a context of preservation of general condition.
Pelvic ultrasound: two latero-uterine masses with vegetations. (fig. 1)
On pevian CT scan: Two endometriotic cysts, one of which is an 11cm compressive inter-utero-rectal cyst and the other is a 5cm left supra-latero-uterine cyst (fig. 2)
The patient underwent exploratory laparotomy with exploration:
• multiple parieto-epiploic and parieto-intestinal adhesions
• presence of a cystic formation in the posterior wall of the vagina: punctured (whitish fluid)
• opening of the cyst wall with drainage of the contents and partial cystectomy with biopsy of the cystic wall
• 2nd cystic formation of 5 cm adherent to the rectum without invasion with partial cystectomy given the adherent state
Anatomopathological study:
• Rectal cyst: invasive papillary and micropapillary serous ADK, well-differentiated with solid squamous territory in favor of adeno-squamous carcinoma
• 2.5 cm vaginal cyst: invasive serous papillary and micropapillary ADK
• 0.7 cm vaginal cyst: invasive serous papillary and micropapillary ADK
• Collection of endometriotic fluid: reaction with a few atypical cells
• Collection of endometriotic fluid: reaction fluid the patient received 6 courses of chiomiotherapy: pacli/carbo
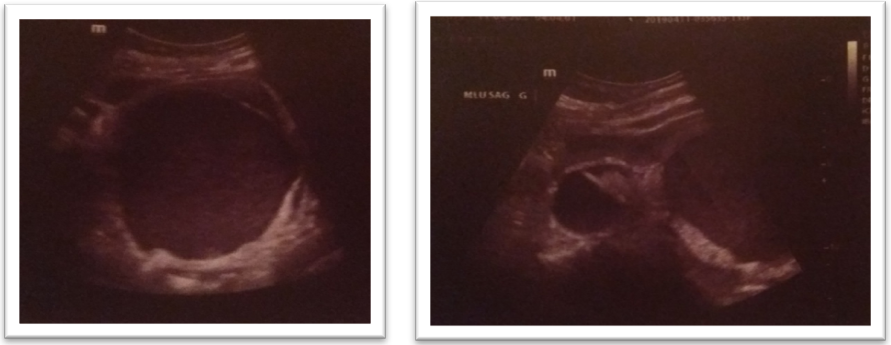
Figure 1: Ultrasound image of two latero-uterine masses
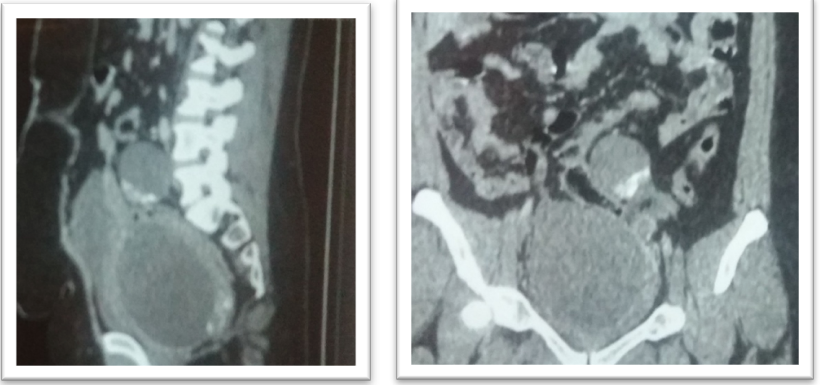
Figure 2: CT image of two endometriotic cysts
Discussion
The diagnosis of papillary adenocarcinoma of the vagina is based on precise histopathological criteria, including arborized papillary structures lined with atypical, sometimes mucosecretory, glandular epithelium [3]. This histological type may be observed in DES-related cases, but also in cases where no etiological factor has been identified, particularly in elderly women [4].
Immunohistochemistry is essential to distinguish a primary vaginal adenocarcinoma from a secondary metastasis, particularly rectal. Expression of CK7, CK20, CDX2 or PAX8 is often helpful in determining tumour origin [5].
Papillary adenocarcinoma of the rectum, on the other hand, is characterized by a predominantly villo-papillary exophytic architecture, sometimes suggestive of a degenerated tubulo-cellular adenoma [6]. Its invasive potential and aggressiveness may vary, but it generally has a better prognosis than mucinous or poorly differentiated forms [7].
The co-existence of papillary adenocarcinoma in both locations raises the question of a single primary tumor with secondary dissemination, or of two synchronous primitivities. This differential diagnosis is based essentially on comparative histology, immunohistochemistry and complete imaging. In some cases, only the clinical course or response to treatment can determine the diagnosis [8].
Treatment is based on an individualized approach. In the case of a primary vaginal tumour, surgical excision may be proposed if size and location allow, possibly supplemented by external radiotherapy or brachytherapy [9]. For adenocarcinomas of the rectum, carcinological surgery (such as low anterior resection or abdominoperineal amputation) combined with neoadjuvant radiochemotherapy is the norm [10]. In the presence of two sites, multidisciplinary consultation is essential to establish the optimal therapeutic sequence.
Prognosis depends on a number of factors: degree of differentiation, depth of invasion, lymph node involvement and response to treatment. The rarity of these cases makes it difficult to establish standard recommendations, hence the importance of reporting each clinical observation to enrich the scientific literature.
Conclusion
Papillary adenocarcinoma of the vagina, especially when associated with rectal cancer of the same histological type, presents a diagnostic and therapeutic challenge. Distinguishing between primary and metastatic disease is essential to guide management. A multidisciplinary approach, including anatomopathology, imaging and oncology, is essential to ensure appropriate treatment. Because of its rarity, each published case contributes to a better understanding of this singular entity.
Reference
- Herbst AL, Ulfelder H, Poskanzer DC. Adenocarcinoma of the vagina: association with maternal diethylstilbestrol therapy. N Engl J Med. 1971;284(16):878–81. [PubMed.]
- Pai RK, Jayachandran P, Koong AC, et al. Histologic subtypes of colorectal adenocarcinoma: morphologic features and molecular correlates. Am J Surg Pathol. 2008;32(3):413–24. [PubMed.]
- Nucci MR, Young RH, Clement PB. Papillary adenocarcinoma of the vagina: a clinicopathologic analysis. Int J Gynecol Pathol. 1997;16(1):38–46. [Ref.]
- Dargent D, Mathevet P, Roy M, et al. Vaginal adenocarcinoma without DES exposure: a rare and controversial entity. Gynecol Oncol. 1996;63(1):53–6. [Ref.]
- Mhawech-Fauceglia P, Herrmann FR, Mickel RA. CK7 and CK20 expression in tumors: a diagnostic value. Appl Immunohistochem Mol Morphol. 2007;15(3):248–53. [Ref.]
- Shia J, Ellis NA, Paty PB, et al. Papillary adenocarcinoma of the colon and rectum: features and classification. Am J Clin Pathol. 2004;122(4):582–8. [PubMed.]
- Verhulst J, Ferdinande L, Demetter P, Ceelen W. Prognostic implications of histological subtypes in colorectal cancer. Virchows Arch. 2015;466(4):337–49. [Ref.]
- Lamovec J, Bracko M. Multiple primary malignancies: diagnostic criteria and challenges. Ann Diagn Pathol. 2004;8(3):191–6. [Ref.]
- Piver MS, Hempling RE, Barlow JJ. Management of vaginal adenocarcinoma: surgery, radiation and outcomes. Obstet Gynecol. 1985;65(3):316–20. [PubMed.]
- Sauer R, Becker H, Hohenberger W, et al. Preoperative versus postoperative chemoradiotherapy for rectal cancer. N Engl J Med. 2004;351(17):1731–40. [PubMed.]