>Corresponding Author : Benhaddouga Khadija
>Article Type : Case Report
>Volume : 5 | Issue : 7
>Received Date : 04 July, 2025
>Accepted Date : 14 July, 2025
>Published Date : 18 July, 2025
>DOI : https://doi.org/10.54289/JCRMH2500132
>Citation : Khadija B, Abdouni A, Moustatir M, Cheikh N, Houssine B, et al. (2025) Desmoid Fibromatosis of the Breast: 1 Case Report and Review of the Literature. J Case Rep Med Hist 5(7): doi https://doi.org/10.54289/JCRMH2500132
>Copyright : © 2025 Khadija B, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Case Report | Open Access | Full Text
1Resident Physician, Department of Gynecology and Obstetrics, at Ibn Rochd University Hospital, Casablanca, Morocco
2Professor in the Department of Gynecology and Obstetrics at the Ibno Rochd University Hospital in Casablanca, Morocco
*Corresponding author: Benhadouga Khadija, Resident Physician, Department of Gynecology and Obstetrics, at Ibno Rochd University Hospital, Casablanca, Morocco
Abstract
Aggressive fibromatosis (desmoid tumour) of the breast is a rare tumour thataccounts only for 0.2% of primary breast tumours. This is a benign mesenchymal tumour that develops from muscular fasciae and aponeuroses. It is characterized by its local evolution and its tendency to relapse without metastasizing. Wide radical resection should be attempted whenever possible. Positive margins at resection and reoperation are associated with a high risk of local recurrence. The role of radiotherapy and of medical treatments especially antiestrogens remains unclear.
Keywords: Desmoid Tumor; Fibromatosis; Breast Cancer; Local Recurrence
Introduction
Desmoid tumour (syn. aggressive fibromatosis, nonmetastasing fibrosarcoma) is a rare benign fibroblastic proliferative disease. It can occur anywhere in the body: most common places are extremities, abdominal wall and intraabdominal cavity. Desmoid tumour is found in only 0.2% of breast tumours [1]. It may be sporadic, but also it may occur after surgical trauma, implantation of silicone breast implants or may be associated with Gardner’s syndrome [2]. Most cases of breast fibromatosis are reported in female, however it may occur in male [2,3].
Breast desmoid tumour presents as firm, painless and movable mass [4]. Nipple, skin retraction may be seen [2,4]. Clinically and radiologically it may mimic breast carcinoma [3]. However, conclusive diagnosis is made after histopathological examination of the lesion. Surgery, radiotherapy, chemotherapy, hormonal therapy may be used for the treatment of desmoids tumour [1,4-6]. Radical surgical excision is the treatment of choice [5].
Case Report
51-year-old patient; primigravida primiparous; with a history of a congenital malformation of the left upper limb; operated on at the age of 25 for trauma to the dorsal spine by osteosynthesis; with the notion of taking oral contraception for two years; always in period of genital activity; operated 2 years ago for neo of the right breast from which she benefited from a right patey with reduction of the contralateral breast; the result of the anatomopathological study of the right breast: presence of a 4 cm infiltrating mammary carcinoma; grade III of SBR has immunohistochemistry corresponds to a Luminal B phenotype, without lymph node metastasis on 20 lymph nodes removed ; in the left breast presence of a fibrous mastopathy without signs of malignancy
The post-operative suites are marked by necrosis of the left areola-nipple plaque for which having benefited from a necrosectomy then she received 6 courses of adjuvant chemotherapy based on antracycline and cyclophosphamide and 25 radiotherapy sessions on the chest wall with a total dose of 50 GY and tamoxifen citrate hormone therapy
A year later she consulted for a nodule in the left breast in which the clinical examination found a nodule of 2 x 2cm at the level of the QSI of the left breast mobile in relation to the 2 planes without inflammatory signs or associated nipple discharge and without axillary adenopathy fig 1.

Figure 1: Nodule in the left superior-internal quadrant, without opposing inflammatory signs
An echo-mammography was performed, objectifying a highly suspicious pre-pectoral lesion in the superior-internal quadrant of the left breast., examination classified BIRADS 5 of the ACR on the left fig 2.
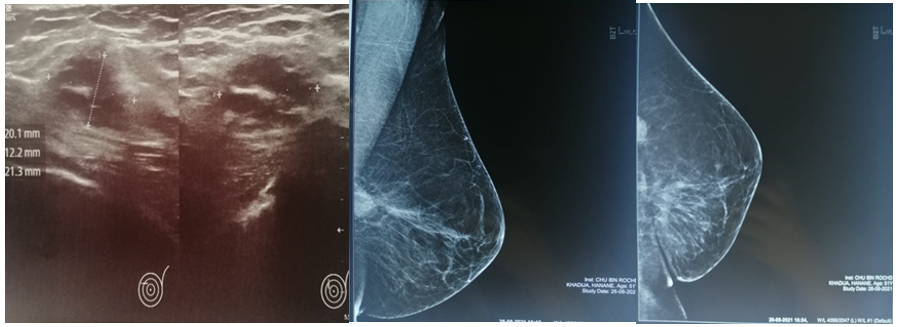
Figure 2: Echo-mammography: was objectifying a pre-pectoral lesion in the superior-internal quadrant of the left breast. , examination classified BIRADS 5
Trucut biopsy was performed with the result: Histological appearance suggestive of mammary desmoid fibromatosis absence of obvious signs of malignancy.
An enlarged lumpectomy was performed: the result of the anathomopathological study: morphological appearance compatible with a deep fibromatosis of the desmoid type, borderline deep limit at less than 1 mm.
The file was discussed in RCP oncogynecology the decision is in favor of a surgical revision with sufficient margins see a possible mastectomy.
The patient underwent a left mastectomy fig 3; the postoperative follow-up was unremarkable fig 3.

Figure 3: Left mastectomy surgical specimen
Discussion
Desmoid fibromatosis of the breast is a benign but locally aggressive tumor characterized by infiltrative fibroblastic proliferation with no [7].
Clinically, fibromatosis of the breast most often manifests itself in young to middle-aged women as a firm, poorly bounded, sometimes painful nodule, which may cause skin retraction or deformation of the breast, mimicking a malignant tumor [8]. Imaging, particularly mammography and ultrasound, shows lesions with a spiculated appearance, without typical calcifications, making the radiological diagnosis unspecific [9].
Diagnosis of certainty is based on histological examination with immunohistochemical study. Fibromatosis presents a proliferation of spindle-shaped cells in a collagenous stroma, with infiltration of adjacent tissues, but without significant nuclear atypia or mitosis. Positive expression of nuclear beta-catenin is a key argument for diagnosis [10]. Other markers such as CD34, S100 or desmin are usually negative, which helps in the differential diagnosis with other fibroblastic or myofibroblastic tumors.
The treatment of choice remains surgical excision with healthy margins. However, local recurrence rates are high, up to 25-30%, particularly in cases of positive or incomplete margins [11]. Conservative surgery is preferable when possible without compromising functional and aesthetic outcome. Recent developments in therapeutic approaches have made it possible to consider active surveillance or medical treatments (anti-inflammatories, tamoxifen, imatinib) in selected cases, particularly for unresectable or recurrent lesions [12].
In short, although benign, desmoid fibromatosis of the breast requires a rigorous multidisciplinary approach. Recognition of this entity is essential to avoid over-treatment and adapt management to its evolutionary potential, while preserving patients' quality of life.
Conclusion
Breast fibromatosis is a very serious pathology rare. she must be known because she can mime, clinically and radiologically, a cancer. Wide surgical excision with margins are the only treatment for this pathology whose evolution is mainly characterized by local recurrence. Radiation therapy is reserved for cases of local recurrence when the surgery is impossible.
Reference
- Wongmaneerung P., Somwangprasert A., Watcharachan K., Ditsatham C. Bilateral desmoid tumor of the breast:case seriesand literature review. International Medical Case Reports Journal. 2016;9:247. [Ref.]
- Erguvan-Dogan B., Dempsey PJ., Ayyar G., Gilcrease MZ. Primary desmoid tumor (extraabdominal fibromatosis) of the breast. American Journal of Roentgenology. 2005;185(2):488–489. [Ref.]
- Muñoz-Atienza V., del Carmen Manzanares-Campillo M., Sánchez-García S., Pardo-García R., Martín-Fernández J. Fibromatosis breast in the male. Case report. Cir Cir. 2013;81:211–213. [PubMed.]
- Ha KY., DeLeon P., Hamilton R. Breast fibromatosis mimicking breast carcinoma. Proceedings (Baylor University. Medical Center. 2013;26(1):22. [PubMed.]
- Seo YN., Park YM., Yoon HK., Lee SJ., Choo HJ., Ryu JH. Breast fibromatosis associated with breast implants. Japanese journal of radiology. 2015;33(9):591–597. [PubMed.]
- Privette A., Fenton SJ., Mone MC., Kennedy AM., Nelson EW. Desmoid tumor:a case of mistaken identity. The breast journal. 2005;11(1):60–64. [PubMed.]
- Glazebrook KN., Reynolds C., Farley DR., et al. Fibromatosis of the breast:imaging findings. AJR Am J Roentgenol. 2008;190(4):1199–1203. [Ref.]
- Haubold RE., Zaren HA., Young PR. Breast fibromatosis:a review of the literature. Ann Surg Oncol. 2010;17(2):577–582. [Ref.]
- Stout AP., Lattes R. Tumors of the Soft Tissues. Atlas of Tumor Pathology. AFIP, Washington DC. 1964. [Ref.]
- Meyers SP., Khazai L., Albarracin CT. Beta-catenin in desmoid-type fibromatosis of the breast:a diagnostic marker. Histopathology. 2012;61(1):94–100. [Ref.]
- Fiore M., Rimareix F., Mariani L., et al. Desmoid-type fibromatosis:a front-line conservative approach to select patients for surgical treatment. Ann Surg Oncol. 2009;16(9):2587–2593. [PubMed.]
- Penel N., Le Cesne A., Bui BN., et al. Imatinib for progressive and recurrent aggressive fibromatosis (desmoid tumors):an FNCLCC/French Sarcoma Group phase II trial with a long-term follow-up. Ann Oncol. 2011;22(2):452–457. [PubMed.]