>Corresponding Author : Benhaddouga Khadija
>Article Type : Case Report
>Volume : 5 | Issue : 6
>Received Date : 02 July, 2025
>Accepted Date : 12 July, 2025
>Published Date : 16 July, 2025
>DOI : https://doi.org/10.54289/JCRMH2500130
>Citation : Benhaddouga K, Mazhour M, Elhodaigui N, Bouchane H, Benchrefi Y, et al. (2025) Parietal Endometriosis in a Post-Hysterectomy Scar: A Diagnostic Challenge and Review of Surgical Management. J Case Rep Med Hist 5(6): doi https://doi.org/10.54289/JCRMH2500130
>Copyright : © 2025 Benhadouga K, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Case Report | Open Access | Full Text
1Resident Physician, Department of Gynecology and Obstetrics, at Ibn Rochd University Hospital, Casablanca, Morocco
2Professor in the Department of Gynecology and Obstetrics at the Ibno Rochd University Hospital in Casablanca, Morocco
*Corresponding author: Benhadouga Khadija, Resident Physician, Department of Gynecology and Obstetrics, at Ibno Rochd University Hospital, Casablanca, Morocco
Abstract
Endometriosis of the abdominal wall is the development of endometrial tissue in the anterior part of the abdomen, usually due to an operation in which the uterus is manipulated. It is a rare entity. It is often misdiagnosed, leading to unnecessary referrals. Gynaecologists and general surgeons need to be aware of this entity to avoid any embarrassment to the patient due to delayed diagnosis. Medical treatment was ineffective. Surgical excision of the mass was the treatment for endometriotic lesions.
Keywords: Endometriosis, Abdomen, Surgical Treatment
Introduction
Endometriosis is defined as the abnormal implantation of functional endometrial epithelium with stroma outside the uterine cavity. It affects women during their reproductive years, with a prevalence of 10%. Its main sites are endopelvic, mainly involving the internal genitalia (ovaries, fallopian tubes, myometrium), the utero-sacral ligaments, the broad ligament and the bladder. Localization in extra-genital organs is less well described. Parietal endometriosis is a rare clinical entity; its occurrence on surgical scars, particularly Pfannenstiel scars, is even less rare (0.03 to 0.4% of all endometrioses), but constitutes the most frequent parietal localization [1]. It is suspected on a number of clinical and radiological grounds but is only confirmed histologically. Parietal endometriosis requires surgical treatment.
Case Report
This is a 44-year-old patient, mother of 2 live children by caesarean section, with history of total inter-annexal hysterectomy in 2018, with anapath: simple hyperplasia without endometrial atypia, 1cm uterine leiomyoma, no signs of malignancy, presenting with chronic pelvic pain, exacerbated 6 months prior to admission, with no urinary or digestive disorders.
On clinical examination: pfannenstiel scar + painful palpation all along the linea alba with perception of a 3cm painful mass founded in the subumbilical adipose panniculus adherent to the rectus abdominis muscle (figure 1).
Pelvic ultrasound: anterior hypogastric parietal mass infiltrating the rectus abdominis muscle measuring 30mm, probably related to an endometriotic graft, hypoechogenic with irregular contour and peripheral vascular pedicle (figure 2).
On pelvic MRI: median subumbilical parietal nodule measuring 5.6 cm, associated with significant infiltration of the parietal fat opposite (figure 3). The patient underwent excision of the parietal mass (figure 4). Pathology: 3.6 cm tissue formation, morphological appearance of endometriosis.

Figure 1: 3cm mass founded in the subumbilical adipose panniculus adhering to the rectus abdominis muscle
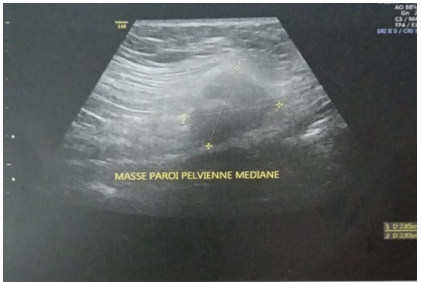
Figure 2: Ultrasound image shows a 3cm parietal mass

Figure 3: Ultrasound image shows a 3cm parietal mass
Discussion
Endometriosis, first described by Rokitansky in 1861, is a common benign gynecological disorder defined as the ectopic implantation of endometrial glands and stroma outside the uterine cavity. Endometriosis is classified as internal or external depending on the involvement of the uterine muscular layer [2-4]. Endometriosis can also be classified as pelvic or extrapelvic, depending on its location. Pelvic endometriosis includes lesions of the fallopian tubes, ovaries and pelvic peritoneum. Extrapelvic endometriosis refers to endometriotic implants found in other areas of the body, including the gastrointestinal tract, lung structures, urinary system, abdominal wall, skin and even the central nervous system.

Figure 4: Surgical part
The mean age at presentation is 31 years [5]. The incidence of the disease is between 6 and 10% of all women, and between 35 and 50% of women with infertility and pelvic pain. The abdominal wall is a rare site of extrapelvic (external) endometriosis, where it usually develops in old surgical scars. Endometriosis has been reported in many types of surgical scars, including scars resulting from endoscopy, Caesarean section, tubal ligation, hysterectomy, inguinal hernia repair, laparotomy and the needle path of third-trimester diagnostic amniocentesis. Scar endometriosis has also been reported in a laparoscopic trocar port site.
The precise etiopathogenesis of endometriosis remains controversial, and many theories have been proposed, including cellular immunity, coelomic metaplasia, implantation or retrograde menstruation, vascular and lymphatic metastases, dissemination and direct transplantation [2,4,6]. Direct transplantation is probably the mechanism responsible for the development of scar endometrioma after caesarean delivery, hysterectomy, appendectomy, laparoscopic trocar or episiotomy [6]. Endometrioma at the trocar port may develop from peritoneal seeding of cells due to pneumoperitoneum or direct contact of the excised lesion with the port tract [2,7].
Clinically: the symptomatology of parietal endometriosis is essentially that of a painful mass with a catamenial character. The cyclical nature of the pain is an important element of orientation, but not indispensable for evoking the diagnosis [1,8]. Lesions located on surgical scars, usually opposite the Pfannenstiel scar, are usually painful masses averaging 2 cm in size. Similar cases have been reported by Hedfi et al, who describe two patients with painful parietal nodules associated with cicatricial endometriosis [9]. A cyclical change in the behaviour of very superficial lesions has also been described, with bleeding and fistulation to the skin [1].
The differential diagnosis of surgical scar endometriosis is broad and is often confused with other pathologies, such as suture granuloma, abscess, inguinal or incisional hernia, soft tissue sarcoma, desmoid tumor, lipoma, metastatic tumor and sebaceous cyst. The pathological diagnosis of endometriosis must therefore be confirmed [2].
Diagnosis is based primarily on clinical arguments. Other diagnostic modalities include ultrasound with color Doppler, CT scan and MRI. On 2D ultrasonography, scar endometriosis may appear as cystic or multicystic, mixed or solid masses, with internal vascularization on power Doppler, but these findings are not specific [10]. Nor does CT play a specific diagnostic role. MRI is a more useful modality for pre-surgical evaluation of deep pelvic endometriosis, infiltration of abdominal wall muscles and subcutaneous tissues [11], but MRI is not cost-effective. Fine-needle aspiration cytology has been used to help establish the diagnosis. However, in cases of suspected incisional hernia, this diagnostic modality should not be used. In addition, recent reports have shown that FNAC fails to diagnose scar endometriosis in many patients [12].
The standard treatment for parietal endometriosis is wide surgical excision from the outset, even if this means performing a parietoplasty to close the aponeurotic dehiscence [7,13]. Medical therapy is also used in the treatment of scar endometriosis and includes non-steroidal anti-inflammatory agents, oral contraceptives, gonadotropin-releasing hormone analogues, aromatase inhibitors and radiofrequency ablation therapy [2].
Post-operative follow-up by a gynecologist is recommended, as there are risks of recurrence that can be successfully managed by re-excision. To prevent the onset of scar endometriosis, it has been suggested that at the end of obstetric and gynaecological surgery, the abdominal wall should be thoroughly cleaned and vigorously irrigated with a high-jet solution prior to closure [14].
Conclusion
Long-term pain should not be taken for granted. A high index of suspicion of cicatricial endometriosis should be present for a swollen surgical scar with cyclic pain. MRI may be useful for preoperative evaluation. Surgical excision is the treatment of choice. Regular follow-up is necessary to detect recurrence.
Reference
- Patil N., Kumar V., Gupta A. Scar endometriosis:a sequel of caesarean section. J Clin Diagn Res. 2014; 8(4):FD09–10. [PubMed.]
- Akbulut S., Sevinc MM., Bakir S., Cakabay B., Sezgin A. Endométriose cicatricielle dans la paroi abdominale:une condition prévisible pour les chirurgiens expérimentés. Acta Chir Belg. 2010; 110(3):303-307. [Ref.]
- Uncu H., Taner D. Endométriose appendiculaire: deux rapports de cas. Arch Gynecol Obstet. 2008; 278(3):273-275. [PubMed.]
- Hensen JH., Van Breda Vriesman AC., Puylaert JB. Endométriose de la paroi abdominale: présentation clinique et caractéristiques d'imagerie avec un accent sur l'échographie. AJR Am J Roentgenol. 2006; 186(3):616-620. [PubMed.]
- Hasan A., Deyab A., Monazea K., Salem A., Futooh Z., Mostafa MA., et al. Évaluation clinico-pathologique des endométriomes de la paroi abdominale retirés chirurgicalement après une césarienne. Ann Med Surg(Londres). 2021; 62:219-224. [PubMed.]
- Chang Y., Tsai EM., Long CY., Chen YH., Kay N. Endométriomes de la paroi abdominale. J Reprod Med. 2009; 54(3):155-159. [Ref.]
- Barbaros U., Iyibozkurt AC., Gulluoglu M., Barbaros M., Erbil Y., Tunali V., et al. Métastase du site du port ombilical endométriosique après laparoscopie. Suis J Obstet Gynecol. 2005; 193(5):1761-1763. [PubMed.]
- Emre A., Akbulut S., Yilmaz M., Bozdag Z. Laparoscopic trocar port site endometriosis:a case report and brief literature review. Int Surg. 2012; 97(2):135–9. [Ref.]
- Mohamed Hedfi & Nada Essid., et al. Endométriose de la paroi abdominale:à propos de deux cas. [PubMed.]
- Wu YC., Tsui KH., Yuan CC., Ng HT. Aspect angiographique Doppler haute fréquence et vitesse du flux microvasculaire dans l'endométriose cicatricielle récurrente. Echographie Obstet Gynecol. 2003; 21:96-97. [PubMed.]
- Lahiri Ashim K., Sharma Kiran., Busiri Naser. Endométriose de la cicatrice utérine de césarienne: à propos d’un cas. Imagerie des femmes. 2008; 18 :66-68. [Ref.]
- Dwivedi AJ., Agarwal SN., Silva YJ. Endométriomes de la paroi abdominale. Creusez Dis Sci. 2002; 47:456–61. [PubMed.]
- Cöl C., Yilmaz EE. Cesarean scar endometrioma:case series. World J Clin Cases. 2014; 16:2(5):133–6. [PubMed.]
- Wakefield SE., Hellen EA. Endométriome du site du trocart après laparoscopie. Eur J Sur. 1996; 162(6):523-524. [PubMed.]