>Corresponding Author : Salma Addi
>Article Type : Case Report
>Volume : 5 | Issue : 5
>Received Date : 17 June, 2025
>Accepted Date : 27 June, 2025
>Published Date : 02 July, 2025
>DOI : https://doi.org/10.54289/JCRMH2500122
>Citation : Addi S, Chyate FZ, Ezahraa TF, Benchrifi Y, Benhessou M, et al. (2025) Phyllodes Tumor in Women: A Case Report. J Case Rep Med Hist 5(5): doi https://doi.org/10.54289/JCRMH2500122
>Copyright : © 2025 Addi S, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Case Report | Open Access | Full Text
1Resident Physician, Department of Gynecology and Obstetrics, at Ibn Rochd University Hospital, Casablanca, Morocco
2Professor in the Department of Gynecology and Obstetrics at the Ibn Rochd University Hospital in Casablanca, Morocco
*Corresponding author: Salma Addi, Resident Physician, Department of Gynecology and Obstetrics, Ibno Rochd University Hospital, Casablanca, Morocco
Abstract
Phyllodes tumours of the breast are uncommon and difficult to treat due to the ambiguity of the diagnosis and the unpredictability of the disease's progression.
Here, we present the case of a 54-year-old female patient who presented with an ulcerating, bourging lesion in her left breast. The diagnosis was confirmed by a histological study. Surgical management was indicated.
Keywords: Phyllodes Tumour, Surgery, Evolution, Prognosis
Abbreviations: WHO: World Health Organization
Introduction
Phyllodes tumours of the breast are rare fibroepithelial tumours that tend to grow rapidly and aggressively, with a high potential for local relapse and/or metastasis [1].
They mainly occur in middle-aged patients (aged 45–50). Adjuvant radiotherapy should be considered in cases of conservative treatment or in the presence of factors predictive of local recurrence [2,3].
This presentation aims to assess the clinical and histopathological characteristics of phyllodes tumours of the breast and the management modalities, as well as the factors that influence the risk of local and/or metastatic recurrence.
Case Report
This is a 54-year-old female patient with no significant medical history, who had her first period at age 13. She is a size II, with a history of exclusively breastfeeding. She presents with an ulcerating, bourging mass in her left breast.
Clinical examination: A 7x6 cm ulcerating-bourging mass covering the entire left breast, which bleeds on contact. The contralateral breast was unremarkable, and the lymph nodes were free (Figure 1).
On mammary MRI, a large breast mass centred on the junction of the external quadrants was observed. It was well-limited with polylobed contours and measured 111x118 mm on the axial section, extending to a height of 125 mm. It was 28 mm from the pectoral muscle, with infiltration of the perilesional fat, and was 6.5 mm thick in the adjacent skin. Axillary adenomegaly measuring10.5 mm with a short axis and fat centre was also observed. The examination was classified as ACR5 on the left and ACR1 on the right (Figure 2).
The biopsy of the mass showed a microscopic appearance that was suggestive of an adenofibromatous formation, with no signs of malignancy.
A clean mastectomy with an extemporaneous examination was performed (see Figure 3). The appearance is consistent with a phyllodes tumour. Histopathological examination revealed: The appearance is compatible with a borderline breast phyllodes tumour (intermediate grade) that has ulcerated the overlying skin. The resection margins on the specimen are healthy.

Figure 1: Image of the Patient's Breasts
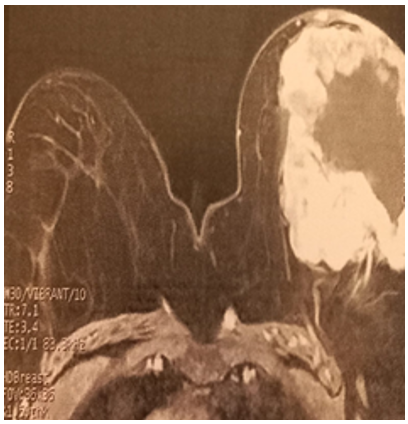
Figure 2: Breast MRI

Figure 3: Surgical specimen
Discussion
Many features of this case are highly unusual for a typical benign phyllodes tumour. Typically, patients present with a firm, well-defined, round, painless mass [4].
In this case, however, the patient presented with an ulcerated, bleeding and infected mass [5].
Phyllodes tumours account for 0.3 to 0.5% of all breast tumours, occur at a later age than fibroadenomas (median age 45 years, 20 years older than fibroadenomas), [6] remain the main differential diagnosis and are characterised by a rapid increase in volume, with an average size varying between 4 and 7 cm [7].
Ultrasound and mammography are the initial paraclinical examinations requested.
On mammography, the contours are usually lobulated and irregularly shaped, with a size greater than 3 cm. Ultrasound translation reveals the following: size > 3 cm, irregular shape, lobulated contours, heterogeneous appearance, hypervascularisation and internal cystic zones. Breast MRI often reveals internal cystic areas [8].
These areas represent fibroepithelial neoplasia, consisting of both an epithelial component and a hypercellular stroma.
According to the World Health Organization (WHO), phyllodes tumours are classified as benign, borderline or malignant based on an assessment of five histological parameters: stromal cellularity, stromal atypia, mitoses, stromal proliferation and tumour margins. Malignant tumours have the potential for distant metastasis, primarily via the blood-borne route.
The usual treatment for a phyllodes tumour is wide excision, but a mastectomy may be more appropriate if the tumour is large or if the histology suggests cancer. Radiotherapy can be effective in certain cases [9].
In this case, the patient underwent a mastectomy due to the extent and ulcerated appearance of the tumour across the entire breast.
The prognosis is good unless metastases (usually pulmonary) are present.
Conclusion
Phyllodes tumours are a type of breast cancer for which the most appropriate treatment for each patient is difficult to determine. For most patients, the treatment of choice is surgical treatment with negative margins of at least 1 cm or mastectomy without axillary lymphadenectomy. However, no difference in survival has been proven.
References
- A V Barrio, et al. Clinicopathologic features and long-term outcomes of 293 phyllodes tumors of the breast. Ann Surg Oncol. 2007;14(10):2961‑2970. [PubMed.]
- M Reinfuss., J Mituś., K Duda., A Stelmach., J Ryś., K Smolak. The treatment and prognosis of patients with phyllodes tumor of the breast: an analysis of 170 cases. Cancer. 1996;77(5):910‑916. [PubMed.]
- L Bernstein., D Deapen., R K Ross.The descriptive epidemiology of malignant cyst sarcoma phyllodes tumors of the breast. Cancer. 1993;71(10):3020‑3024. [PubMed.]
- M Reinfuss., J Mituś., K Duda., A Stelmach., J Rys., K Smolak. The treatment and prognosis of patients with phyllodes tumor of the breast: an analysis of 170 cases. Cancer. 1996;77(5):910‑916. [PubMed.]
- S P Mishra., S K Tiwary., M Mishra., A K Khanna. Phyllodes tumor of breast: a review article. ISRN Surg. 2013;361469. [PubMed.]
- S J Parker., S A Harries. Phyllodes tumours. Postgrad Med J. 2001;77(909):428‑435. [PubMed.]
- M Strode., T Khoury., C Mangieri., K Takabe. Update on the diagnosis and management of malignant phyllodes tumors of the breast. Breast Edinb Scotl. 2017;33:91‑96. [PubMed.]
- L Duman., et al. Differentiation between Phyllodes Tumors and Fibroadenomas Based on Mammographic Sonographic and MRI Features. Breast Care Basel Switz. 2016;11(2):123‑127. [PubMed.]
- L H Rosenberger., et al. Contemporary Multi-Institutional Cohort of 550 Cases of Phyllodes Tumors (2007-2017) Demonstrates a Need for More Individualized Margin Guidelines. J Clin Oncol Off. J Am Soc Clin Oncol. 2021;39(3):178‑189. [PubMed.]