>Corresponding Author : Bouyalik Fadwa
>Article Type : Case Report
>Volume : 5 | Issue : 4
>Received Date : 01 April, 2025
>Accepted Date : 14 April, 2025
>Published Date : 07 May, 2025
>DOI : https://doi.org/10.54289/JCRMH2500116
>Citation : Fadwa B, Leila E, Oumnia EB, Houssine B, Sakher M, et al. (2025) Disseminated Peritoneal Leiomyomatosis: A Rare Entity (A Case Report). J Case Rep Med Hist 5(4): doi https://doi.org/10.54289/JCRMH2500116
>Copyright : © 2025 Fadwa B, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Case Report | Open Access | Full Text
1Resident Physician, Department of Gynecology and Obstetrics, at Ibno Rochd University Hospital, Casablanca, Morocco
2Professor in the Department of Gynecology and Obstetrics at the Ibno Rochd University Hospital in Casablanca, Morocco
*Corresponding author: Bouyalik Fadwa, Resident Physician, Department of Gynecology and Obstetrics, Ibno Rochd University Hospital, Casablanca, Morocco
Abstract
Disseminated peritoneal leiomyomatosis (DPL), or leiomyomatosis peritonealis disseminata, is a sporadic benign disorder characterized by multiple solid nodules of peritoneal smooth muscle that proliferate along the abdominopelvic cavity. The cause of the disease is unknown, although iatrogenic and hormonal stimulation have been suggested as causes. It mainly affects women of reproductive age. Imaging studies are important in determining the extent of lesions and the presence of malignancy. There are no conventional therapeutic guidelines for the treatment of DPL, and therefore the risk of malignant transformation is low. We discuss the case of a 46-year-old woman who had previously undergone laparoscopic hysterectomy and presented 4 years later with numerous peritoneal tumors.The diagnosis of DPL was suspected by computed tomography and magnetic resonance imaging and confirmed by histology.
Keywords: Peritoneal, Leiomyomatosis, Dissemination, Smooth Tumor
Abbreviations: DPL: Disseminated Peritoneal Leiomyomatosis, MRI: Magnetic Resonance Imaging, IVL: Intravenous Leiomyomatosis, BML: Benign Metastatic Leiomyoma, HL: Hereditary Leiomyomatosis
Introduction
Disseminated peritoneal leiomyomatosis is one of a group of smooth muscle tumors of uncertain growth, including diffuse uterine leiomyomatosis, intravascular leiomyomatosis and benign metastasizing leiomyoma [1]. DPL is a rare entity characterized by the appearance of multiple nodules of smooth muscle cells in the peritoneal cavity. First described by Wilson and Peale in 1952 [2]. It is often asymptomatic and discovered fortuitously.
Case Report
A 46-year-old female, with a history of hypertension under treatment, had surgery for uterine leiomyoma 6 years ago, had presented for 2 years a chronic cyclic pelvic pain with no other associated signs. The poor clinical examination and the absence of any abnormality visible on ultrasound led to the performance of an initial magnetic resonance imaging (MRI). Initial magnetic resonance imaging (MRI) revealed moderately enlarged ovaries with multiple follicles of varying size. Two follicles, the right measuring 31 mm in height, 26 mm in width and 21 mm in thickness, and the left measuring 28 mm in width, 19 mm in anteroposterior diameter and 25 mm in height, may correspond to hemorrhagic or endometriosis follicles (figure 1).
The biological markers were at a rate of 28.7 U/ml.
The patient subsequently received 2 courses of DECAPEPTYL 11.25 mg at 3-month intervals.
Given the persistence of symptomatology despite treatment, a decision to perform diagnostic laparoscopy was warranted, whose exploration found superficial and deep chocolate-brown nodules at the level of the Douglas cul de sac, and multiple biopsies were taken (figure 2).
The Anatomopathological examination revealed disseminated peritoneal leiomyomatosis.
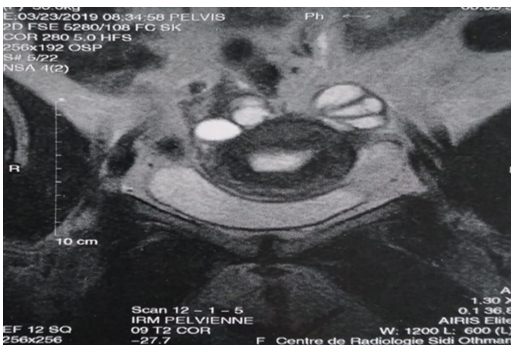
Figure 1: Pelvic MRI image showing hemorrhagic or endometriotic follicles
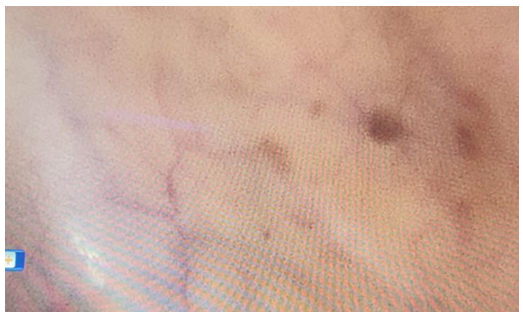
Figure 2: laparoscopic view of the peritoneal cavit.
Discussion
Diffuse peritoneal leiomyomatosis (DPL) is characterized by the presence of numerous small nodules of smooth muscle cell leiomyomas covering the abdominal viscera and peritoneum.
There are four more or less distinct entities of ectopic leiomyoma reported in the literature: intravenous leiomyomatosis (IVL), benign metastatic leiomyoma (BML), disseminated peritoneal leiomyomatosis (DPL) and hereditary leiomyomatosis (HL) [3].
Since its first description by Wilson and Peale in 1952, over 100 cases of DPL have been reported in the literature, including 8 with malignant evolution [2].
The origin of this pathology remains obscure: DPL is thought to be linked to a metaplasia affecting the pluripotent cells of the mesenchymal subperitoneum, and more precisely, the mullerian epithelium [4].
The DPL is most often discovered by chance during surgery, such as caesarean section, laparoscopy or laparotomy. However, it may be accompanied by aspecific symptoms: pelvic pain or heaviness, metrorrhagia, digestive symptoms [4].
The lesion affects young women. It is usually associated with prolonged contraceptive use or pregnancy, and nodule regression is reported when these factors are discontinued. Some cases are associated with hormone-secreting ovarian neoplasms [5]. One study showed the presence of LH (luteinizing hormone) receptors, suggesting a role for gonadotropins in the development of PDL during the menopause [6].
Radiological presentation is highly variable and unspecific. Sometimes in the form of multiple nodules, sometimes as a single mass. On CT-scan, these lesions are strongly enhanced and homogeneous. When the mass is large, there may be hypodense foci corresponding to necrotic-cystic areas [7].
However, the final diagnosis can only be made on histological analysis.
Macroscopically, in PDL, the peritoneal surface, bowel, bladder and uterus are riddled with firm nodules of greyish-white appearance on cross-section, with a few haemorrhagic foci, varying in size from a few millimetres to several centimetres in diameter [8].
Microscopically, these nodules are composed of smooth muscle fibers and may contain myofibroblasts and decidualized cells. They often show no mitoses or only a low mitotic index (less than 3 mitoses/10 fields at × 400 magnification). High mitotic activity, changes in chromatin texture, increased cell density or nuclear pleomorphism raise the suspicion of malignancy. In the literature, immunohistochemical studies show that the only positive markers in LPD are actin, desmin and estrogen and progesterone receptors [2-8].
There is no consensus on either diagnosis or treatment. Treatment must take into account the patient's hormonal status, and whether or not the lesions are symptomatic. Conservative medical treatment with Gn-RH agonists can be proposed to women in the active genital period. Post-menopausal women usually benefit from a complete surgical procedure. In the case of unresectable symptomatic tumours, some authors suggest chemotherapy with carbamazepine or doxorubicin, [9]. Because of the risk of degeneration, a CT scan is recommended, but there is no consensus [2].
The prognosis of LPD is usually good. Indeed, spontaneous regression is frequent after removal of the triggering hormonal factor. With the exception of a few cases of recurrence and eight cases of malignant transformation, which have been reported in the literature [2-8].
Conclusion
Disseminated peritoneal leiomyomatosis is a rare, benign entity whose etiology remains unknown. It is usually diagnosed by chance during surgery, and its macroscopic appearance makes it a diagnosis to be considered in the presence of peritoneal thickening without a primary tumor in a young woman. It is a differential diagnosis not only of peritoneal carcinomatosis, but also of tuberculosis, mesothelioma, lymphoma and leiomyosarcomatosis.
References
- M Gleyze., V Conri., V Brard., J L Brun., C HockéLes. Tumeurs musculaires lisses de croissance incertaine:à propos d’un cas de léiomyomatose péritonéale disséminée Pôle d’Obstétrique Reproduction Gynécologie, Service de chirurgie gynécologique, Centre Aliénor d’Aquitaine, Hôpital Pellegrin, CHU de Bordeaux, France. [Ref.]
- Maya Bucher M., Marc Pusztaszeri M., Hanifa Bouzourene H. La léiomyomatose péritonéale disséminée:profil immunohistochimique et origine. Ann Pa-thol. 2006;26:207-10. [Ref.]
- E Declas et al. La léiomyomatose extra-utérine:revue de la littérature. Gynécologie Obstétrique Fertilité & Sénologie. 2019;47(7-8):582-590. [PubMed.]
- Acid S. et al. Leiomyomatose peritoneale disseminee. Journal de Radiologie. 2006; 10:87(10). [Ref.]
- Tavassoli FA., Norris HJ. Peritoneal leiomyomatosis (leiomyomatosis peritonealis disseminata):a clinicopathologic study of 20 cases with ultrastructural observations. Int J Gynecol Pathol. 1982;1:59-74. [PubMed.]
- Danikas D., Goudas VT., Rao CV., Brief DK. Luteinizing hormone receptor expression in leiomyomatosis peritonealis disseminata.Obstet Gynecol. 2000;95:1009-11. [PubMed.]
- L ROY., SCHMUTZ., Régent. Léiomyomatose péritonéale disséminée. départment de radiologie diagnostique de faculté de medecine et des sciences de la santé de Québec. [Ref.]
- Trabelsi., K Mrad., M Driss., K Ben Romdhane. Léiomyomatose péritonéale disséminée:à propos d’un cas avec étude immunohistochimique S. Laboratoire d’anatomie pathologique, Institut Salah Azaïz. 1006 Bab Saadoun, Tunis, Tunisie. [Ref.]
- Trabelsi., K Mrad., M Driss., K Ben Romdhane. Léiomyomatose péritonéale disséminée:à propos d’un cas avec étude immunohistochimique S. Laboratoire d’anatomie pathologique, Institut Salah Azaïz. 1006 Bab Saadoun, Tunis, Tunisie. [Ref.]