>Corresponding Author : Sabir Soukaina
>Article Type : Case Report
>Volume : 4 | Issue : 8
>Received Date : 05 June, 2024
>Accepted Date : 19 June, 2024
>Published Date : 23 June, 2024
>DOI : https://doi.org/10.54289/JCRMH2400142
>Citation : Soukaina S, Hajar E, Fadwa A, Chehrazad E, Siham N, et al. (2024) Malignant degeneration of benign cystic teratoma of the ovary : A report Case. J Case Rep Med Hist 4(8): doi https://doi.org/10.54289/JCRMH2400142
>Copyright : © 2024 Soukaina S, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Case Report | Open Access | Full Text
1Resident Physician, Department of Gynecology and Obstetrics, at Ibno Rochd University Hospital, Casablanca, Morocco
2Professor in the Department of Gynecology and Obstetrics at the Ibno Rochd University Hospital in Casablanca,Morocco
3Resident Physician, Department of anatomopathology, at Ibno Rochd University Hospital, Casablanca, Morocco
*Corresponding author: Sabir Soukaina ,Resident Physician, Department of Gynecology and Obstetrics, Ibno Rochd University Hospital, Casablanca, Morocco
Abstract
Malignant degeneration of benign cystic teratoma of the ovary is a rare complication occurring mostly during post-menopausal period. The malignant transformation of the benign teratoma has no specific clinical nor radiological, nor biological signs. The treatment is surgical and preferentially similar to that of epithelial tumors of the ovary. We report an observation of a squamous cell carcinoma developed on a mature cystic teratoma of the ovary, in a patient aged 59 years, revealed by the final histopathological exam of an adnexectomy with a mature teratoma of the ovary.
Keywords: Malignant degeneration, Cystic benign teratoma, epithelial tumors, Ovarian tumor
Abbreviations: CT: Computed Tomography
Introduction
Teratomas of the ovary are the most common germ cell tumours, with mature teratomas of the ovary occurring in 10-20% of cases [1]. Malignant transformation of one or more components of mature teratomas is rare, occurring in around 1-2% of cases [2]. Carcinogenesis may lead to squamous cell carcinoma in 80% of cases, adenocarcinoma or, rarely, sarcoma [3]. Diagnosis is most often made after anatomopathological study of the surgical specimen, as the clinical symptomatology and radiological presentation of malignant transformation are devoid of specificity. This poses a major problem in the initial surgical management, which may not be optimal due to lack of knowledge of the carcinogenesis [4]. We report an observation concerning a 59-year-old woman presenting with chronic pelvic pain, whose imaging revealed a mature teratoma of the ovary, which was surgically treated and revealed squamous cell carcinoma on the surgical specimen.
Case Report
The patient was 59 years old, nulliparous, menopausal, menarche at age 13, with no particular pathological history. She consulted for chronic pelvic pain, which had been evolving for 6 months. Clinical examination revealed a mobile left latero-uterine mass with a groove separating it from the uterus.A CT scan of the abdomen and pelvis revealed a left ovarian mass measuring 75x55x60 mm, with mixed density, fat and tissue, with well-limited oval calcifications, suggestive of an ovarian teratoma (Figure 1). Tumor markers were normal. A left adnexectomy under laparotomy was performed (Figure 2).

Figure 1. CT image of a mature teratoma of the left ovary
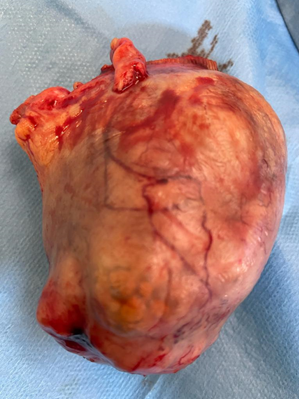
Figure 2. Surgical specimen of a left adnexectomy with a mature teratoma of the ovary
Macroscopic examination revealed a smooth-walled, renitrating mass containing hairs, sebum and an ossified zone (figure 2). Final histological examination confirmed the diagnosis of a moderately differentiated squamous cell carcinoma on a mature teratoma of the ovary (figure 3 and 4).

Figure 3. Histological sections stained with hematoxylin-eosin (x20): mature pluritissular teratoma containing respiratory-type epithelial lining (a), smooth muscle tissue (b), keratinizing squamous lining (c), adipose tissue (d).

Figure 4. Histological section stained with hematoxylin-eosin (x40): Carcinomatous proliferation arranged in clumps and guts, cells with marked cytonuclear atypia (a), with presence of keratin beads (b).
The decision of the multidisciplinary consultation staff was to complete the operation with a total hysterectomy and contralateral adnexectomy, which returned without malignant proliferation, no adjuvant treatment was indicated, biannual surveillance was carried out and no recurrence was observed.
Discussion
Approximately 1-3% of mature teratomas of the ovary develop carcinoma, and this association accounts for only 0.17-1% of all ovarian carcinomas [3]. A mature teratoma of the ovary is defined as a dermoid cyst in which a carcinoma has developed on one of its mature components [5].
The age of onset of this cancer in our patient was 59 years, which corresponds to the average age of onset described by several authors, which is 54 years [3]. Approximately 75% of dermoid cysts become cancerous in the postmenopausal period [6].
The clinical presentation is not specific, but similar to that of benign ovarian cysts, dominated by pelvic pain [3]. Radiologically, some authors suggest that signs suggestive of malignancy include adhesion to neighbouring structures, increased wall thickness, the presence of necrosis and haemorrhage, size greater than 99 mm, an increase in the size of a dermoid cyst in the menopausal period, or any growth greater than two centimeters per year during genital activity, should also raise suspicion of malignant transformation of a dermoid cyst [7].
Among the biological elements studied, only squamous cell carcinoma (SCC) analysis could point to malignant transformation of a dermoid cyst. However, a low level of this marker does not rule out carcinogenesis [3]. The diagnosis of dermoid cyst carcinoma is often difficult preoperatively, and only histological examination can confirm the diagnosis [5]. The management of cancerized teratomas of the ovary is not yet well codified, and given the small number of cases studied, it is a truly controversial subject [7].
In women of childbearing age and for early stages, unilateral adnexectomy without adjuvant treatment is recommended. In post-menopausal women, on the other hand, extensive surgery is recommended [3]. The role of chemotherapy and radiotherapy has yet to be determined [8].
The prognosis of mature cancerized teratomas depends closely on clinical stage and histological type [9]. Five-year survival is around 50% for stage I squamous cell carcinomas, 25% for stage II tumours and 12% for stage III tumours [10].
Conclusion
Cancerized dermoid cysts of the ovary are rare, occurring in post-menopausal women. Confirmatory diagnosis is histological, and is made on the final surgical specimen. Given that 80% of mature teratomas of the ovary are detected during the period of genital activity, and that cancerized teratomas are diagnosed in the postmenopausal period, carcinogenesis would therefore be linked to exposure of unresected mature teratomas to numerous carcinogenic factors.
References
- Ribeiro G, Hughesdon P, Wiltshaw E. Squamous carcinoma arising in dermoid cysts and associated with hypercalcemia: a clinicopathologic study of six cases. Gynecol Oncol. 1988;29:222-30. [PubMed.]
- Yamanaka Y, Tateiwa Y, Miyamoto H, Umemoto Y, Takeuchi Y, Katayama K, et al. Preoperative diagnosis of malignant transformation in mature cystic teratoma of the ovary. Eur J Gynaecol Oncol. 2005;26(4):391-4. [PubMed.]
- Rim SY, Kim SM, Choi HS. Malignant transformation of ovarian mature cystic teratoma. Int J Gynecol Cancer. 2006;16:140-4. [PubMed.]
- Denguezli W, et al. Transformation maligne sur tératome mature kystique de l’ovaire. Med Maghreb. 2008;157:32-6. [Ref.]
- Chbani L, et al. Transformation maligne épithéliale d’un tératome mature de l’ovaire : à propos d’un cas. Rev Franc Lab. 2008;407:99-102. [Ref.]
- Mori Y, Nishii H, Takabe K, et al. Preoperative diagnosis of malignant transformation arising from mature cystic teratoma of the ovary. Gynecol Oncol. 2003;90:338-41. [PubMed.]
- Argoitia X, Duga I, Labeyrie E, Toledo L, Couteau C, Querleu D. Dégénérescence des kystes dermoïdes: à propos d’un cas de transformation maligne. Obstet Fertil. 2007;35(10):1005-8. [PubMed.]
- Dos Santos L, Mok E, Iasonos A, Park K, Soslow RA, Aghajania, et al. Squamous cell carcinoma arising in mature cystic teratoma of the ovary: a case series and review of the literature. Gynecol Oncol. 2007;105:321-4. [PubMed.]
- Tseng C, Chou H, Huang K, Chang T, Liang C, Lai C, et al. Squamous cell carcinoma arising in mature cystic teratoma of the ovary. Gynecol Oncol. 1996;63:364-70. [PubMed.]
- Kashimura M, Shinohara M, Hirakawa T, Kamura T, Matsukuma K. Clinicopathologic study of squamous cell carcinoma of the ovary. Gynecol Oncol. 1989;34:75-9. [PubMed.]