>Corresponding Author : Elomri Hajar
>Article Type : Case Report
>Volume : 4 | Issue : 9
>Received Date : 19 June, 2024
>Accepted Date : 04 July, 2024
>Published Date : 16 July, 2024
>DOI : https://doi.org/10.54289/JCRMH2400141
>Citation : Hajar E, Fadwa B, Imane Z, Errih L, Oumnia E, et al. (2024) Ovarian Torsion During A 14 Weeks Pregnancy: A Case Report. J Case Rep Med Hist 4(9): doi https://doi.org/10.54289/JCRMH2400141
>Copyright : © 2024 Hajar E, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Case Report | Open Access | Full Text
1Resident Physician, Department of Gynecology and Obstetrics, at Ibn Rochd University Hospital, Casablanca, Morocco
2Professor in the Department of Gynecology and Obstetrics at the Ibn Rochd University Hospital in Casablanca, Morocco
*Corresponding author: Elomri Hajar, Resident Physician, Department of Gynecology and Obstetrics, Ibno Rochd University Hospital, Casablanca, Morocco
Abstract
Ovarian torsion during pregnancy is a relatively uncommon emergency presenting with acute pelvic pain, the torsion of the ovary during pregnancy is a rare complication. Clinical symptoms are often non-specific. Pelvic ultrasound remains the gold standard investigation. Laparoscopy is recommended in young pregnancies. We report the case of a 23-year-old female patient, pregnant at 14 weeks amenorrhoea, who presented with pain in the right iliac fossa and who was found to have a torsion of the right ovary on pelvic ultrasound. Exploration showed an increased torsion of the right ovary around the pedicle at 360°, an oophoropexy was performed.
Keywords: Pelvic pain, Ovarian torsion, pregnancy, Oophoropexy
Introduction
Ovarian torsion is the twisting of an ovary on its ligamentous supports. It is a rare condition with very high morbidity. If it occurs during pregnancy, it can lead to fetal mortality and affect the patient's fertility prognosis by compromising blood supply. However, the diagnosis remains difficult due to the ascending ovary in the last months of pregnancy, which can simulate other surgical emergencies such as acute appendicitis, cholecystitis or acute pyelonephritis. Any acute pelvic pain in a pregnant woman should raise the suspicion of ovarian torsion. Radiological and biological data can be used to support the diagnosis, but it must be based on a careful history and physical examination. Conservative treatment is the rule, provided the diagnosis is made early and treatment is prompt to avoid maternal and fetal complications. The aim of this study is to describe the clinical aspect and the interest of early management to preserve ovarian capital and the conditions that allow this.
Ovarian capital and the conditions that allow pregnancy to be carried to term postoperatively. The impact on quality of life is significant and can be severe.
Case Report
Mrs Z.E., 23 years old, second gravida primiparas, mother of a vaginal birth, with no particular pathological history, a regular cycle and an idea to take clomiphene citrate eight months before her admission.
She presented to the obstetric emergency department with pelvic pain of two days' duration and amenorrhoea of 14 weeks' duration. Clinical examination revealed a conscious patient with stable haemodynamics and respiratory status.
The abdominal examination showed a tenderness of the right uterus.
Gynaecological examination showed an enlarged uterus with right-sided latero-uterine pain. Pelvic ultrasound showed a progressive pregnancy at 14 weeks of amenorrhoea (Figure 1), with a tumefied right ovary of 88 cm2 with multiple follicles in a peripheral arrangement. The stroma was not vascularised by Doppler, with visualisation of a spiral turn at the hilum. We also found a small amount of free pelvic fluid (Figure 1,2).
As laparoscopy was not possible due to a technical problem, a laparotomy was indicated by the obstetric team. Exploration revealed a very enlarged right ovary measuring 10 cm, multifollicular, 360° around the pedicle, without necrosis or suspicious tumour appearance (Figure 3). The left ovary was also enlarged, measuring 5 cm, multifollicular, without torsion (Figure 4). The uterus was enlarged and gravid. Detorsion of the right ovary was performed, followed by ovarian revascularisation and oophoropexy. No blood loss was noted.
The postoperative course was uncomplicated, the pain had disappeared and the patient was discharged on the third postoperative day. An ultrasound scan after one month showed a developing pregnancy with 19 weeks of amenorrhoea, and the ovaries had returned to their normal size.
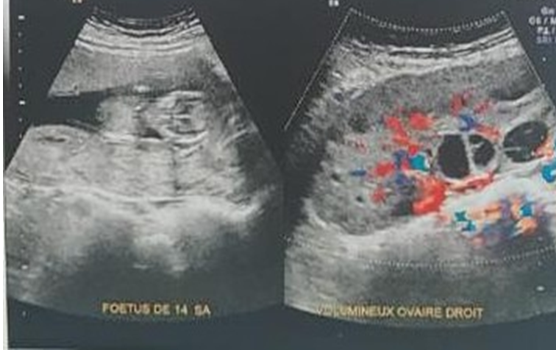
Figure 1. 14-week pregnancy associated with a torsion of the right adnexa.

Figure 2. Right ovarian torsion and twisting on its ligamentous supports

Figure 3. Enlarged right ovary’s torsion around the pedicle 360°.

Figure 4. Enlarged left ovary, without torsion.
Discussion
Ovarian torsion in pregnancy is a rare complication. It causes high maternal morbidity and fetal mortality if not treated promptly. [1] Its incidence varies between 3 to 5 per 10,000 pregnancies [1,2]. Between 8 and 28% of torsions occur during pregnancy, [3,4] particularly in the first trimester, but can be diagnosed at any time [4]. Ovarian torsion is more common on the right side because on the left side the sigmoid colon limits the mobility of the left ovary [1,5].
Clinical symptoms are often non-specific, consisting of pelvic pain, lateral, acute in onset, associated with nausea and vomiting. The clinical diagnosis is difficult due to the anatomical changes of the gravid uterus, the concomitant elevation of the ovaries in the abdominal position and the frequency of the other usual differential diagnoses, notably miscarriage, retroplacental haematoma or uterine rupture.
Pelvic ultrasound remains the gold standard, although it is not very effective in detecting positive signs of torsion. It allows the indirect signs of ischaemia to be sought and the differential diagnosis to be ruled out. The interruption of the blood supply leads to reactive oedema, resulting in an increase in ovarian volume [6,7]. The increase in the number of cortical follicles is a non-specific aspect, often seen in torsion of a healthy adnexa, and is due to fluid transudation secondary to ovarian congestion [7, 8]. As far as magnetic resonance imaging is concerned, it is a complementary investigative technique of the same interest as ultrasound, offering greater precision.
Adnexal torsion is a surgical emergency; therefore laparoscopy is recommended when the gestational age is less than 17 weeks, with an insufflation pressure between 8 and 12 mmHg, an adapted position of the trocars and gentle mobilisation of the uterus [9].
The therapeutic option depends on the appearance of the adnexa ten minutes after detorsion [10]. Conservative treatment is recommended in the case of complete or partial recovery after detorsion [11]. In case of friable black necrotic lesions after detorsion, adnexectomy is preferred. Other authors recommend conservative treatment despite uncertain vitality because of the possible recovery of ovarian function [12].
Oophoropexy is recommended to prevent recurrence and in cases of ovarian ligament malformation [13]. The corpus luteum provides the hormonal synthesis necessary to maintain pregnancy until the appearance of the placenta. However, drainage or excision of the cyst may result in loss of the pregnancy. Therefore, some obstetricians prefer to add progesterone therapy to maintain the pregnancy until the placenta can provide its hormonal function [14].
Conclusion
The diagnosis of ovarian torsion is a clinical one. It must be suspected in any pregnant woman presenting with sudden abdominal-pelvic pain. It is a diagnostic and therapeutic emergency to avoid the prognosis of fertility. Treatment must be as conservative as possible, consisting of detorsion of the adnexa. Oophopexy should not be performed systematically unless there is an immediate recurrence of torsion or a malformation of the ovarian ligaments.
References
- Lentz GM, Lobo RA, Gershenson D, et al. Comprehensive Gynecology. 6th ed. Mosby, Inc; 2012. pp. 383-432. [Ref.]
- Kumari I, Kaur S, Mohan H, et al. Adnexal masses in pregnancy: a 5-year review. Aust N Z J Obstet Gynaecol. 2006;46(1):52-4. [PubMed.]
- Oelsner G, Cohen SB, Soriano D, et al. Minimal surgery for the twisted ischaemic adnexa can preserve ovarian function. Hum Reprod. 2003;18(12):2599-602. [PubMed.]
- Boughizane S, Naifer R, Hafsa A, et al. Laparoscopic management of adnexal tumors after the first trimester of pregnancy. J Gynecol Obstet Biol Reprod (Paris). 2004;33(4):319-22. [PubMed.]
- Sasaki KJ, Miller CE. Adnexal torsion: review of the literature. J Minim Invasive Gynecol. 2014;21(2):196-202. [PubMed.]
- Graif M, Shalev J, Strauss S, et al. Torsion of the ovary: sonographic features. AJR Am J Roentgenol. 1984;143(6):1331-4. [PubMed.]
- Pansky M, Smorgick N, Herman A, et al. Torsion of normal adnexa in postmenarchal women and risk of recurrence. Obstet Gynecol. 2007;109(2 Pt 1):355-8. [PubMed.]
- Zweizig S, Perron J, Grubb D, et al. Conservative management of adnexal torsion. Am J Obstet Gynecol. 1993;168(6 Pt 1):1791-5. [PubMed.]
- Bider D, Mashiach S, Dulitzky M, Kokia A, Lipitz S, Ben-Rafael Z. Clinical surgical and pathologic findings of adnexal torsion in pregnant and non-pregnant women. Surg Gynecol Obstet. 1991;173(5):363-6. [PubMed.]
- Oelsner G, Bider D, Goldenberg M, Admon D, Mashiach S. Long-term follow up of the twisted ischemic adnexa managed by detorsion. Fertil Steril. 1993;60:976-9. [PubMed.]
- Shalev E, Peleg D. Laparoscopic treatment of adnexal torsion. Surg Gynecol Obstet. 1993;176:448-50. [PubMed.]
- Tepper R, Lerner-Geva L, Zalel Y, Shilon M, Cohen I, Beyth Y. Adnexal torsion: the contribution of color Doppler sonography to the diagnosis and the postoperative follow-up. Eur J Obstet Gynecol Reprod Biol. 1995;62(1):121-3. [PubMed.]
- Way S. Ovarian cystectomy of twisted cysts. Lancet. 1946;2:47-8. [PubMed.]
- Nichols DH, Julian PJ. Torsion of the adnexa. Clin Obstet Gynecol. 1985;28:375-80. [PubMed.]