>Corresponding Author : Vijendra Patle
>Article Type : Case Report
>Volume : 4 | Issue : 6
>Received Date : 18 March, 2024
>Accepted Date : 02 May, 2024
>Published Date : 06 May, 2024
>DOI : https://doi.org/10.54289/JCRMH2400128
>Citation : Patle V, Kaur D, Rathod A, Sandeep VS and Dayapati S. (2024) Acute Liver Failure with Intracerebral Hemorrhage in Dengue Fever: A Rare Clinical Presentation. J Case Rep Med Hist 4(6): doi https://doi.org/10.54289/JCRMH2400128
>Copyright : © 2024 Patle V, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Case Report | Open Access | Full Text
1Junior Resident, Department of General Medicine GMCH, Chandigarh, India
2Assistant Professor, Department of General Medicine GMCH, Chandigarh, India
*Corresponding author: Vijendra Patle, Junior Resident, Department of General Medicine GMCH, Chandigarh, India
Abstract
Dengue is the major cause of arthropod-borne viral disease in the world. It presents with high fever, headache, rash, myalgia, and arthralgia and it is a self-limiting illness. Severe dengue can occur in some cases resulting in dengue hemorrhagic fever (DHF) and dengue shock syndrome (DSS). We present a case of a young patient aged 25-year-old male who presented with fever, jaundice, decreased urine output for 5 days, and altered mental status for the last 1 day. After investigation, he was diagnosed with dengue fever and later developed sepsis-induced acute liver failure with acute kidney injury. The patient was treated with intravenous antibiotics and hemodialysis. Plasmapheresis was done in view of acute liver failure. Gradually patient condition improved and he gained consciousness. But later on, the patient developed spontaneous intracerebral hemorrhage (ICH) and the patient succumbed to his illness after 2 days of developing ICH. ICH is a very rare and atypical manifestation in the case of severe dengue patients, research for effective treatment is crucial now.
Abbreviations: DHF: Dengue Hemorrhagic Fever, DSS: Dengue Shock Syndrome, ICH: Intracerebral Haemorrhage, ALF: Acute Liver Failure, NAC: N- Acetyl Cysteine, PLEX: Plasma Exchange, ICU: Intensive Care Unit, Hb: Haemoglobin, TLC: Total Leucocyte Count, ALT: Alanine Aminotransferase, AST: Aspartate Aminotransferase, PT: Prothrombin Time, INR: International Normalised Ration
Introduction
Dengue fever stands as the predominant mosquito-borne arboviral illness worldwide, with transmission facilitated by the Aedes aegypti and Aedes albopictus mosquitoes, endemic to Southeast Asia, including India. Dengue virus is a single stranded enveloped RNA virus it has four serotypes namely DEN 1 to DEN 4. It manifests across a broad clinical spectrum, ranging from asymptomatic cases to classic dengue fever, severe dengue haemorrhagic fever, and the potentially fatal dengue shock syndrome [1,2]. In its severe manifestation, this disease can affect multiple organs such as the liver, brain, and kidneys, often culminating in fatal consequences. The pathogenesis driving severe illness is not completely understood, yet there exists evidence suggesting that cytokine storms and elevated viremia levels correlate with heightened organ involvement. Among the affected organs, the liver is frequently impacted, demonstrating a range of effects from asymptomatic elevation of liver enzymes to the onset of acute liver failure (ALF) [1,2]. Nonetheless, various mechanisms have been elucidated, encompassing direct viral damage, immunological injury, and hypoxic injury stemming from diminished hepatic perfusion during shock [3]. Liver function showed significant improvement with N- Acetyl Cysteine(NAC), Plasma Exchange(PLEX), and other supportive measures.
Case Presentation
A 25 year old male, resident of Punjab presented to medicine emergency in altered sensorium state for 1 day having history of fever associated with chills and rigor moderate to high grade for 5 days, jaundice and decreased urine output for 3 days. No history of any intoxication was present.
On examination, the patient was drowsy and not oriented to time, place, and person with GCS- E3V2M4. Bilateral pupils were equal and reactive to light and no signs of meningitis were present. Yellowish discoloration of sclera and skin along with ecchymosed patches in the right gluteal region were present. The patient was tachypnoeic with a respiratory rate of 30/minute SpO2 92% under VM @ 6L/min and tachycardia with a pulse rate of 123/min, although he was normotensive with BP-122/80 mmHg at presentation. Per abdomen examination was soft with no organomegaly. On auscultation, bilateral normal vesicular breath sounds were present with no added sounds. The patient had no history of alcohol intake, hepatotoxic medicines like Paracetamol and NSAIDs, or herbal medicines known to cause liver injury. Other causes of ALF like Hepatitis (HAV, HBV, HCV, HEV) and Other tropical infections like Malaria, Leptospira, and scrub Typhus were negative in this case.
The patient was intubated in view of poor GCS on 1st day after admission to the hospital and shifted to the Intensive Care Unit (ICU). Routine investigations including cultures were sent. Full Blood count showed Haemoglobin(Hb) of 13.1 g/dl, Haematocrit 38.8%, Total LeucocyteCount(TLC) of 23.3k cells/dl, and platelets of 25k/dl. Liver Biochemistry showed Alanine aminotransferase (ALT) – High and Aspartate aminotransferase (AST) – high with Total bilirubin of 5.5 g/dl. Prothrombin Time(PT)-24 and International normalized ratio (INR)- 1.8. Renal function tests showed urea- 94, and creatinine- 4.3. Dengue IgM came out to be positive. NCCT Head was normal on the 1st day of admission. The patient was managed conservatively with intravenous fluids and broad-spectrum antibiotics. Four units of RDP were also transfused. Serum ammonia levels came out to be raised by 161 (normal range 90-140) i.e. TABLE- 01. He had coagulopathy along with raised bilirubin, transaminitis, and hepatic encephalopathy grade IV features - suggestive of Acute Liver Failure (ALF). The patient was started on NAC infusion for a total duration of 21 hours. The patient was on hemodialysis every alternate day as he was anuric since his presentation with rising serum creatinine levels. The patient was planned for plasmapheresis after a multidisciplinary team meeting on 3rd day of admission and completed 2 cycles of plasmapheresis on alternate days. There is a significant improvement in sensorium and his liver functions and coagulopathy were managed with fresh frozen plasma i.e. FIG 02-03. The patient's condition gradually improved and he gained consciousness. He was gradually weaned off from mechanical ventilation and extubated on the 5th day of admission. But suddenly patient condition deteriorated on the 7th day of illness with GCS E2V2M2 and was reintubated. Repeat NCCT Head was done s/o right-sided Intracerebral hemorrhage with intraventricular hemorrhage as shown in FIG-01 and the patient succumbed after the 9th day of illness.
The patient had no history of alcohol intake, hepatotoxic medicines like Paracetamol and NSAIDs, or herbal medicines known to cause liver injury. Other causes of ALF like Hepatitis (HAV, HBV, HCV, HEV) and Other tropical infections like Malaria, Leptospira, and scrub Typhus were negative in this case.
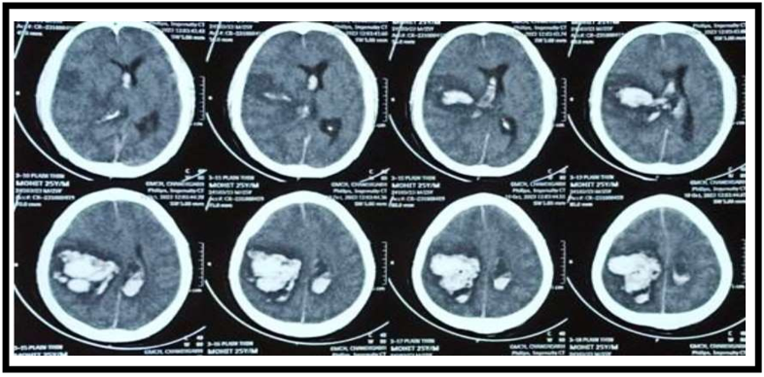
Figure 1: NCCT head of patient s/o right sided ICH and IVH

TABLE 1: A summary of laboratory parameters of the patient during the hospital stay. (Day 1 being the day of admission) Hb- Haemoglobin, Hct- hematocrit (in percentage), TLC- Total leucocyte count, Bil- Bilirubin, ALP- Alkaline phosphatase, ALT- Alanine transaminase, AST- Aspartate transaminase, LDH-Lactate dehydrogenase, PT- Prothrombin time, PTI- Prothrombin time index, INR- International normalised ratio, S.NH3- serum ammonia
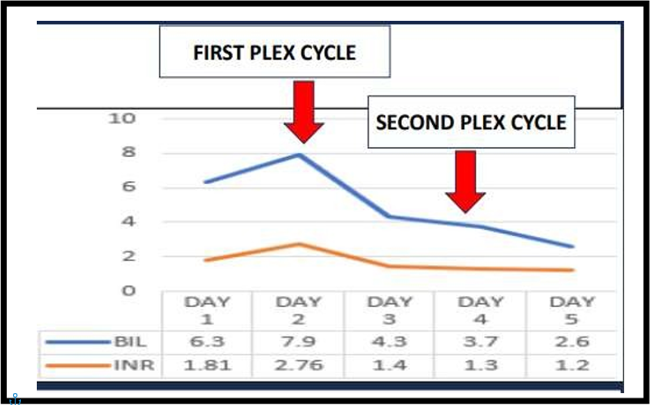
Figure 2: Showing improvement in the Bilirubin and INR after PLEX
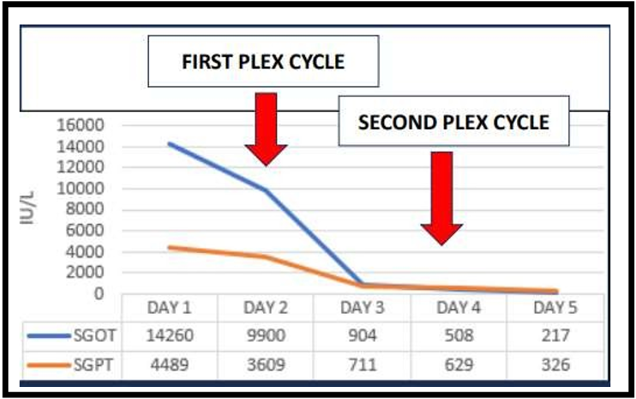
Figure 3: Showing improvement in Transaminases after PLEX cycle
Discussion
Dengue fever is rapidly emerging as the most widespread mosquito-borne viral ailment globally. Annually, approximately 50 million cases of dengue occur across approximately 100 tropical and subtropical nations. A staggering 70% of individuals at risk of contracting dengue reside in Southeast Asia and the Western Pacific region. Endemic to Southeast Asia, including India, dengue is caused by the Dengue virus, a member of the Flaviviridae family and the genus Flavivirus. This RNA virus possesses an envelope and encodes both structural and non-structural proteins. Structural proteins consist of the capsid, precursor membrane, and envelope, while the virus encodes seven non-structural proteins, including NS1, utilized as a diagnostic antigen in the early stages of the illness. Dengue virus is categorized into four serotypes, namely DENV 1–4 [2].
Studies have demonstrated that the Dengue virus prompts apoptosis in human hepatocyte cells. Although the precise mechanism driving this hepatic injury remains elusive, there is speculation surrounding T cell-mediated host immunity and the associated cytokine storm, often termed a cytokine"Tsunami.” [1].
Acute liver failure frequently triggers multi-organ dysfunction, leading to cardiovascular instability, renal failure, cerebral edema, and ultimately, irreversible shock-induced fatalities. Coagulopathy, alongside ensuing bleeding complications, also contributes significantly to the pathogenesis [1,3]. Treatment strategies like NAC administration and preventing hypoperfusion or dengue shock syndrome could potentially aid in managing the condition, but their universal effectiveness remains unproven. In the current landscape, there are limited therapeutic interventions accessible for severe liver disease [4].
Liver transplantation stands as the sole established approach to salvage individuals afflicted with acute liver failure(ALF). However, due to the scarcity of donors, extending liver transplantation to all ALF patients is unfeasible. Consequently, there is a pressing need to explore novel strategies aimed at halting the progression of hepatocyte damage. Plasma Exchange (PLEX) has demonstrated efficacy in modulating innate immunity, thereby enhancing liver transplant-free survival rates and, consequently, overall outcomes [4,5].
This case illustrates that dengue fever has the potential to induce acute liver failure even in the absence of obvious bleeding and Dengue shock syndrome, and can lead to markedly elevated hepatic transaminase levels. NAC infusion and PLEX showed significant improvement in liver function in our case. Intracranial hemorrhage (ICH) is one of the rare and fatal complications of the central nervous system involvement by dengue as a part of expanded dengue syndrome [6]. In this case, the patient developed spontaneous ICH at a platelet count of around fifty thousand which is very rare, therefore research for effective guidelines and treatment is crucial and demanding now.
References
- Arunpriyandan V, Sundaresan KT. (2022) Fulminant Hepatic Failure in Dengue Fever Without Plasma Leakage: A Case Report. Cureus. 14(4): e23964. [Ref.]
- Suganthan N, Sakthilingham G, Kumanan T. (2020) Dengue fever complicated with acute liver failure: A case report of expanded dengue syndrome and literature review. SAGE Open Med Case Rep. 8: 2050313X20913428. [Ref.]
- Dalugama C, Gawarammana IB. (2017) Dengue hemorrhagic fever complicated with acute liver failure: a case report. J Med Case Rep. 11(1): 341. [Ref.]
- Kotoh K, Kato M, Kohjima M, Nakamuta M, Enjoji M. (2010) A new treatment strategy for acute liver failure. World J Hepatol. 2: 395-400. [Ref.]
- Larsen FS, Schmidt LE, Bernsmeier C, et al. (2016) High-volume plasma exchange in patients with acute liverfailure: an open randomised controlled trial. J Hepatol. 64: 69-78. [PubMed.]
- Singh A, Balasubramanian V, Gupta N. (2018). Spontaneous intracranial hemorrhage associated with dengue fever: An emerging concern for general physicians. Journal of family medicine and primary care. 7(3): 618-628. [Ref.]