>Corresponding Author : Sushant Babbar
>Article Type : Case Report
>Volume : 4 | Issue : 4
>Received Date : 13 Feb, 2024
>Accepted Date : 26 Feb, 2024
>Published Date : 29 Feb, 2024
>DOI : https://doi.org/10.54289/JCRMH2400119
>Citation : Babbar S, Kaur R and Kumar A. (2024) Breast Hydatid Masquerading as Breast Neoplasm: Report of 2 Cases. J Case Rep Med Hist 4(4): doi https://doi.org/10.54289/JCRMH2400119
>Copyright : © 2024 Babbar S, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Case Report | Open Access | Full Text
1Senior Resident, Department of Radiodiagnosis, Indira Gandhi medical college, Shimla, India
2Senior Resident, Department of Obstetrics and Gynecology, Post Graduate Institute of, Medical Education and Research, Chandigarh, India
3Senior Resident, Department of Radiodiagnosis, Post Graduate Institute of Medical Education and Research, Chandigarh, India
*Corresponding author: Sushant Babbar, Senior Resident, Department of Radiodiagnosis, Indira Gandhi medical college, Shimla, India
Abstract
Hydatid cyst a parasitic disease which is caused by larval stages of cestodes of Echinococcus family (“Echinococcus granulosus” or “Echinococcus multilocularis”). Most commonly it involves liver and lungs; however it can occur¬ in unusual locations like spleen, psoas muscles, mesentery, ovary, inguinal region and breast. Breast hydatid are very rare and are often masquerade as tumoral lesion of breast. In literature, few reports of breast hydatid are published and nearly all cases have been diagnosed post operatively. Purpose is to bring clinical and radiological character of this rare entity to the clinician’s and radiologist’s awareness.
Introduction
Hydatid disease is parasitic disease which is “endemic” in various parts of the world. The causative agent for the disease is larval stages of cestodes of Echinococcus family (“Echinococcus granulosus” or “Echinococcosis multilocularis”). Humans are the accidental who acquires the infection by ingestion of eggs that hatches in the small bowel and release oncosphere that penetrates intestinal wall and migrates through circulatory system to various organs. Most common site of infection is liver (60%) and lungs (30%), however hydatid disease has been encountered at very uncommon locations like kidney (2.5%), spleen (1.5%), muscles (1%) [1]. Only few case reports of breast hydatid (0.27%) [2] are published most of which are diagnosed postoperatively [3].
In this case report we are presenting 2 cases of who presented with lump breast and were finally diagnosed with hydatid disease breast.
CASE 1
40 year old married female presented to Surgery OPD with chief complaints of painless swelling since 3 years in left breast which increased in size over a period of time. On palpation the lump was of size 6X5 cm in upper quadrant of breast extending behind nipple areolar complex and was well defined, firm in consistancy, non tender and mobile. There was associated lymph node enlargement in axilla. Rt breast was normal. On mammography (Fig 1) there was high density oval well circumscribed mass lesion seen. No associated micro or macrocalcification. Nipple areolar complex normal. On USG this mass was completely cystic with fine internal echoes. No internal septation present (Fig 2). Another cystic lesion was detected in liver on ultrasound (Fig 3) with thick laminated membranes and further evaluated with CECT to rule out disseminated hydatid disease. On workup echinococcus IGG serum level was raised with titres upto 9.07. Surgical excision of hydatid from breast and liver was done (Fig 4).
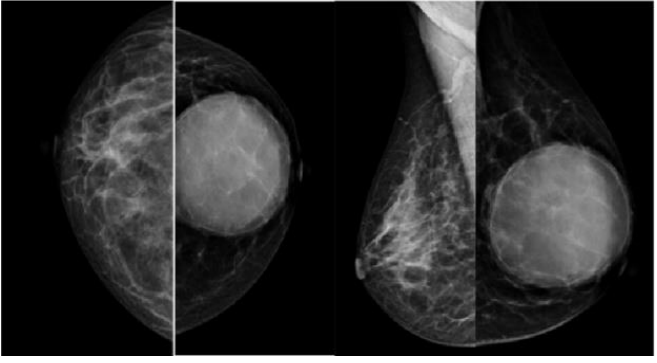
Figure 1: Mammography images a.) Craniocaudal b) MLO view depicting high density well defined rounded lesion of size 6.2x5.8 cm seen in the left breast in retroareolar region. This lesion was classified under BIRADS category II.

Figure 2: USG image well defined anechoic unilocular cystic lesion in retroareolar region with posterior acoustic enhancement was seen in left breast
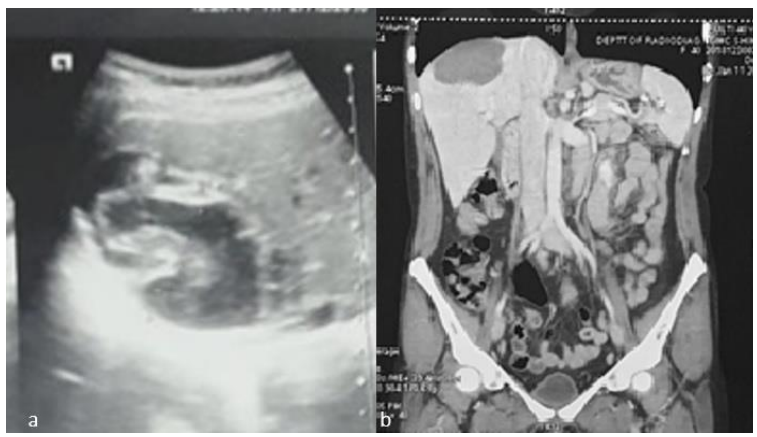
Figure 3: a) USG abdomen shows heterogeneously hypoechoic lesion of size 7.3x5 cm seen in segment VII and VIII of Rt lobe of liver reaching upto subdiaphragmatic surface with presence of multiple laminated membranes b) CECT images shows well defined hypodense lesion in segment VII & VIII of liver measuring 6.2x6.8 cm with CC extent of 5.3 abutting sub diaphragmatic surface with CT value of 35-55 HU with thin fine septations with in it.
Case 2 75 year old female who presented to the surgery opd with c/c of lump rt. breast x 6months. on clinical examination it was mobile, non tender well defined mass in retroreolar area. No palpable axillary lymphadenopathy. Ultrasound evaluation revealed multiloculated cystic lesion with septation. No increased vascularity/ calcification seen (Fig 5). Provisional diagnosis of breast carcinoma was kept considering age of the patient. FNAC was done which showed protoscolices with inflammatory cells in background suggesting possibility of hydatid cyst. Laboratory workup revealed raised echinococcus IGG serum level to 8.76. Surgical excision of the hydatid cyst was done (Fig 6).

Figure 4: Intraoperative fondings shows exicion specimen of the breast hydatid which mimics Gross specimen of Liver hydatid.
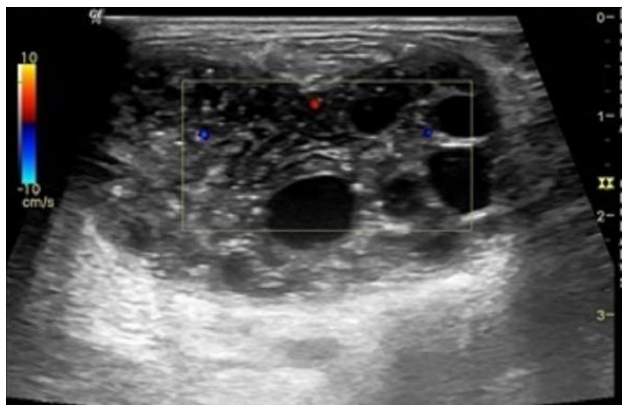
Figure 5: USG shows heterogenous lesion with multiple septation and cystic areas.

Figure 6: Post operative specimen of breast hydatid.
Discussion
Hydatid disease is parasitic disease which is endemic in various parts of the world. The causative agent for the disease is larval stages of cestodes of Echinococcus family (Echinococcus granulosus or Echinococcosis multilocularis). Definite host is usually dog but can be other carnivore with sheeps being the most common intermediate hosts. Humans may become intermediate host/ accidental host when come in contact with definite host who acquires the infection by ingestion of eggs that hatches in the small bowel. The released hexacanth embryo passes through intestinal wall into portal circulation and migrates through circulatory system to various organs.
Liver is most ommonly involved because it acts as a first filter and stops about 75% of embryos, while lung being the second filter which stops about 10% of embroys is second most common site of infestation. Only about 15% embryos are free to develop cysts in other organs of the body. One of the study by Barret and Thomas found involvement of liver by cysts in 60% followed by 30% in lungs and rarely involving kidneys and heart in 2.5%, pericardium & bone in 2 %, 1.5% in spleen, 1% in muscle, and 0.5% in brain [1]. Hydatid disease can involve virtually any organ with reported incidence of 0.27% for breast hydatid of all cases [2]. The breast can be a primary site or part of a disseminated hydatidosis [3]. Typically, the patient presents with painless breast lump as in our case, which increases slowly in size without regional lymph node involvement. It generally affects women between 30 and 50 years of age and can other malignant or non malignant lesion of breast. Breast hydatid cyst should be included in differential diagnosis of breast lumps especially in endemic areas to help diagnose the disease in preoperative period [3,4]. Preoperative confirmation by fine needle aspiration cytology can be done where scolexes, hooklets or laminated membrane can be identified [5]. FNAC is safe procedure with no major reported complications. Radiologic or serologic evaluation also help towards diagnosis however, both of these are not definitive. “Vega et al” described that mammogram may show a high density well circumscribed mass, with the characteristic ring shaped structures inside the mass in over penetrated view which is strongly suggestive of breast hydatid cyst [6]. The ultrasound and Magnetic Resonance Imaging are helpful diagnostic tools”. Majority of the cases reported in literature are diagnosed postoperatively unlike in these cases where preoperative diagnosis of hydatid was made which helped proper planning of the surgical excision.
The definite treatment for hydatid disease of breast is complete excision. However, recurrence of cysts have been reported postoperatively in upto 10% of patients. Use of anti helminthic medication (albendazole) may help in decreasing the recurrence rate of hydatid cyst disease in post operative period [7,8].
Conclusion
Preoperative diagnosis of breast hydatid is challenging, however hydatid disease of breast should be kept as differential diagnosis in cystic lesions of breast in patients of endemic region. Ultrasonography can give a clue about the diagnosis. Fine needle aspiration cytology can help in its preoperative diagnosis. Albendazole help decrease recurrence after surgical removal.
Conflict of Interest: None
Financial Disclosure: None
Disclaimer: This material was not presented/published elsewhere. Informed consent was obtained for publishing images
References
- Saeed M, Jarbou MD, Wasfi M, Salaita MD, Mohammad A, et al. (2007) Isolated hydatid cyst of breast: a case report. JRMS. 14(1): 64-65. [Ref.]
- Taori KB, Mahajan SM, Hirawe SR, Mundhada RG. (2004) Hydatid disease of the breast. Indian journal of radiology and imaging. 14(1): 57-60. [Red.]
- Farrokh D. (2000) Hydatid cysts of the breast: a report of three cases. Irn J Med Sci. 25(1&2): 72-75. [Ref.]
- Langer JC, Rose DB, Keystone JS, Taylor BR, Langer B. (1984) Diagnosis and management of hydatid disease of the liver. Ann Surg. 199(4): 412-417. [Ref.]
- Sagin H.B, Kiroglu Y, Aksoy F. (1994) Hydatid cyst of the breast diagnosed by fine needle aspiration biopsy. A case report. Acta Cytol. 38(6): 965-967. [PubMed.]
- Mirdha B, Biswas A. (2001) Echinococcosis: presenting as palpable lumps of breast. Indian J Chest Allied Sci. 43(4): 239-241. [PubMed.]
- Dagli AF, Ozercan MR, Kocakoc E. (2006) Hydatid cyst of the breast mimicking inflammatory carcinoma and mastitis. J Ultrasound Med. 25(10): 1353-1356 [PubMed.]
- Farrokh D, Hashemi JB, Zandi B. (2007) Primary hydatid cyst of the breast: A case report. Iran J Radiol. 4(3): 159-162. [Ref.]