>Corresponding Author : Eslam A Tabl
>Article Type : Case Report
>Volume : 4 | Issue : 2
>Received Date : 18 Jan, 2024
>Accepted Date : 31 Jan, 2024
>Published Date : 04 Feb, 2024
>DOI : https://doi.org/10.54289/JCRMH2400106
>Citation : Hosny GA, Tabl EA and Elnaser AA. (2024) Metacarpal Lengthening: A Case Report Including Lengthening of Three Metacarpals. J Case Rep Med Hist 4(2): doi https://doi.org/10.54289/JCRMH2400106
>Copyright : © 2024 Hosny GA, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Case Report | Open Access | Full Text
1Professor of orthopedic surgey, Benha University, Egypt
2Assistant professor of orthopedic surgey, Benha University, Egypt
3Assistant lecturer of orthopedic surgey, Benha University, Egypt
*Corresponding author: Eslam A Tabl, Assistant professor of orthopedic surgey, Benha University, Egypt
Abstract
Introduction: Using distraction osteogenesis in metacarpal lengthening has been well documented in pediatric patients but has a limited trials in older patients. Fewer studies have assessed the success of the procedure through outcome measure scores.
The aim of this study is to report a case of distraction osteogenesis of three metacarpals in skeletally mature adult with amputated middle three fingers and patient’s perspective on her satisfaction through the Michigan hand outcomes questionnaire [1].
Keywords: Metacarpal; Lengthening; Callotasis
Introduction
Bone lengthening continues to be a real challenge to both the patient and the orthopedic surgeon. Although it is not a difficult operative problem, there is a long and exhausting postoperative commitment which can jeopardize early good results [2].
Post-traumatic digital deficiency will result in partial or even complete loss of digital opposition function and the contour of the affected hand. Digital lengthening is one of the effective reconstructive surgeries that improve opposition function and hand shape [3].
In children, good results have been achieved with callotasis regardless of the original pathology or the lengthening required. Previous studies assessed lengthening in children and young adults with congenital shortening, whereas in children with traumatic shortening the technique remains controversial regarding several points3 such as the site of osteotomy (metaphyseal vs. diaphyseal), the rate of distraction the time to start distraction, the use of bone graft and phalangeal versus metacarpal lengthening in traumatic cases where the amputation stump is very short [4].
Bone lengthening for aesthetic reasons for normal or short bones has been reported recently. The ethical principles and psychological factors have to be taken into consideration. Psychiatric evaluation is mandatory for all patients to exclude body dysmorphic disorder. It is mandatory to have detailed preoperative psychological analysis to rule out any psychiatric illness which might affect the patient’s ability to make a sensible decision. A single counselling session of limited time may not be enough to have fair appraisal of patient sanity. It would be wise to arrange several meetings between the patient and previously treated patients as part of the preoperative preparation program to give them a real example of the difficulties to be expected before reaching their goal [2].
Metacarpal lengthening was firstly described by Mansoor in 1969. In 1967, Matev presented his experience with satisfactory results on many cases and he suggested metacarpal lengthening for thumb amputations [5].
The purpose of this study is to report a case of distraction osteogenesis of three metacarpals in skeletally mature adult with amputated middle three fingers and patient’s perspective on her satisfaction through the Michigan hand outcomes questionnaire [1].
Case report
Thirty years old female presented to us with old complete amputation of her middle three fingers of left hand since she was 2 years old after crushing trauma (Fig 1).
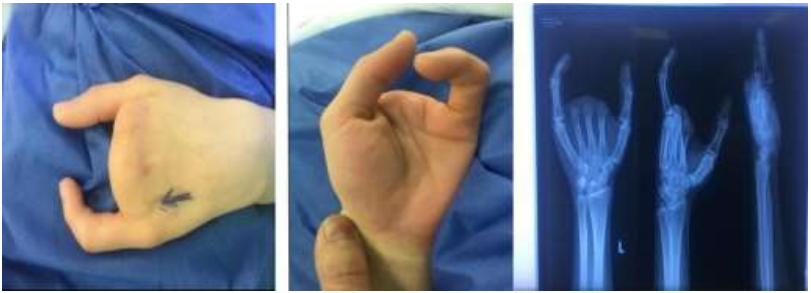
Figure 1. Clinical photos and x rays at time of presentation.
The patients can move her thumb and little fingers without limitations, she seeking for cosmetic purpose and function if available.
We decided to do metacarpal lengthening of middle 3 metacarpals using the principle of Callotasis of the hand and then a web-plasty operations, first we started with 4th metacarpal using uniplaner external fixator with distractor as the patient’s well as she was afraid of the procedure (Fig. 2).
The extent of distraction in short bone lengthening depended on the development of pain, sensory, and vascular changes in lengthened fingers. We did not think that the soft tissue around the metacarpals (transverse carpal ligament) has been influential on the magnitude of distraction, we can distract up to 100% of original length (Fig. 3).
Distraction-lengthening started after 10 days, Gradual lengthening was begun at a rate of 0.25 mm twice daily. We used passive dynamization, in which patients loosened the fixator clamps in the morning and tightened it at night which allowed micromovement of the callus to enhance bone formation.

Figure 2. Steps of 4th metacarpal lengthening and final distraction achieved.

Figure 3. X-ray after fixator removal at 8 months post operative and clinical photo after pin track healing.
After the first set the patient satisfaction was high and encouraged us to proceed to next steps, so combined lengthening of 2nd and 3rd metacarpals at one set planned, patient sent to physiotherapy prior to 2nd operation. Unfortunately a fracture of 4th metacarpal while physiotherapy occur, but this didn’t change the plan and we proceed to 2nd operation and take the advantage of 4th metacarpal breakage to enhance bone formation and that is what happened (Fig 4, 5).

Figure 4. Fracture of 4th metacarpal while in physiotherapy.

Figure 5. Distraction osteogenesis of 2nd, 3rd metacarpals with healing of 4th metacarpal fracture with accepted angulation.
The external fixator of 3rd metacarpal removed on 6 months post operative then 1 month later another device removed, we could achieve 80% of 3rd metacarpal length in distraction (Fig. 6,7).

Figure 6. At the left: the pre-operative x rays, to the right: last x rays after lengthening and show about 80% of 3rd metacarpal length achieved.

Figure 7. Last clinical photo post web-plasty operation
Discussion
Various techniques such as osteotomy and intercalary bone grafting have been described in treating short metacarpals. Acute lengthening poses various disadvantages such as inadequate lengthening, morbidity to the donor site and neurovascular compromise. By gradual distraction, greater bone length can be achieved and fewer complications are observed.
Callotasis of the hand has several advantages: it is less invasive than other techniques as bone grafting is unnecessary, gradual distraction is possible, joint mobilization can be performed during treatment, and sensation is maintained. Disadvantages include longer period of treatment and perhaps the need for complicated and bulky instrumentation [4].
Possible complications have been reported in distraction osteogenesis such as pin tract infection, pin loosening, bowing of the lengthened bone, premature consolidation, callus fracture and non-union. However, we did not experience any of the major complications described except mild angulation in 4th metacarpal.
In our case, 28 mm or 80% of the pre-operative bone length was achieved, yet such complications were not observed, there was no consensus regarding the optimal rhythm and frequency of lengthening. Most authors recommended lengthening between 0.5 mm to 1.0 mm per day; two to four daily lengthening [6]. In our case, two daily lengthenings of 0.25 mm each giving 0.5 mm per day was appropriate to us as no complications were noted.
According to the Michigan hand outcomes questionnaire we achieved good results in scale 5 (aesthetics) and scale 6 (satisfaction) but fair in other scales, but this results met with patient’s ambitions, and also the unique case of lost digits and use three metacarpal lengthening to achieve patient’s aesthetic needs make this work difficult to compare with other authors achievements in hand function as they deal with lost part of digits or metacarpals with intact digits.
In conclusion, distraction osteogenesis is safe and easy. Limb lengthening is a rapidly developing field of orthopaedic surgery. Currently it is a standard procedure with predictable results, and indications have been extended to include the upper extremities and cosmetic lengthening. We recommend that stability of the fixation, preservation of the periosteum, pin tract care and patient’s education and compliance should be emphasized.
Conflict of Interest: The authors declare that they have no conflict of interest
Funding: The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval and consent: A full informed consent taken from patient, with ethical approval from institution taken.
References
- Chung KC, Pillsbury MS, Walters MR, Hayward RA. (1998) Reliability and validity testing of the Michigan hand outcomes questionnaire. J Hand Surg Am. 23: 575-587. [PubMed.]
- Gamal A, Hosny. (2020) Limb lengthening history, evolution, complications and current concepts. J Orthop Traumatol. 21: 3. [PubMed.]
- Zhenyu Ding, Xiaozhong Zhu, Kai Fu, and Xianyou Zheng. (2017) Digital Lengthening to Treat Finger Deficiency: An Experience of 201 Digits in 104 Patients; BioMed Research International. 2017: 4934280. [Ref.]
- Gamal Ahmad Hosny, Wael Abdelaziz Kandel. (2012) Distraction lengthening by callotasis of traumatically shortened bones of the hand. J Trauma Acute Care Surg. 72(6): 1676-1680. [PubMed.]
- Firdous Khan, Asif Shah and Najiullah Khan. (2012) Metacarpal and Phalangeal Lengthening of the Hand. Utility of Distraction Osteogenesis. Professional Med J. 19(1): 15-22. [Ref.]
- Khan F, Khan N, Shah A. (2012) Metacarpal and phalangeal lengthening of the hand; utility of distraction osteogenesis. Professional Med J. 19(1): 15-22. [Ref.]