>Corresponding Author : Bendahou H
>Article Type : Case Report
>Volume : 3 | Issue : 1
>Received Date : 26 Dec, 2022
>Accepted Date : 16 Jan, 2023
>Published Date : 18 Jan, 2023
>DOI : https://doi.org/10.54289/JCRMH2300105
>Citation : Bendahou H, Ettagmouti Y, Abouriche A, Maaroufi A, Haboub M, et al. (2023) Cardiotoxicity Due to Docetaxel Rare But it Exists: About a Case and Literature Review. J Case Rep Med Hist 3(1): doi https://doi.org/10.54289/JCRMH2300105
>Copyright : © 2023 Bendahou H, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Case Report | Open Access | Full Text
1Department Of Cardiology. Ibn Rochd University Hospital of Casablanca, Morocco
2Department Of Oncology. Ibn Rochd University Hospital of Casablanca, Morocco
*Corresponding author: Bendahou H, Department Of Cardiology. Ibn Rochd University Hospital of Casablanca, Morocco
Abstract
Despite the development of anti-cancer treatments, cancers remain among the most common causes of morbidity and mortality. The prognosis depends on the natural evolution of the disease in the first instance, but also on the increasingly frequent side effects of anticancer treatments.
Cardio oncology is an emerging sub-specialization in its own right that deals with these complications.
We report the case of an 80-year-old patient with prostate cancer who received 8 courses of docetaxel and developed left ventricular dysfunction related to docetaxel cardiotoxicity.
This case is among the few in the literature elucidating docetaxel cardiotoxicity in the form of heart failure, which should prompt consideration of echocardiographic monitoring in patients receiving taxanes.
Keywords: Docetaxel; Cardiotoxicity; Cardio Oncology
Introduction
Docetaxel is a new taxoid antineoplastic agent, widely used to treat breast and prostate cancer, especially the metastatic forms [1].
Since docetaxel has its actions by stabilizing microtubules, it can induce contractile dysfunction as a cardiotoxic agent [1].
The clinical case presented below, is a rare form of this type of cardiotoxicity in a patient followed for prostate neoplasia.
This type of cardiotoxicity is rare and negligible, but can be serious, requiring close monitoring and management.
Case Report
We report the case of an 80-year-old patient, with no particular cardiovascular risk factors, followed in oncology unit for prostatic adenocarcinoma of Gleason score 6, locally advanced, with infiltration of periprostatic fat and seminal vesicles associated with lymphadenopathy, bilateral urethrohydronephrosis and secondary bone localizations at level D9, D12, and L1.
The patient underwent a pulpectomy and an endoscopic resection of the prostate with a double J probe mounted by his urologist and was then referred to oncology for additional care.
Chemotherapy was indicated and a cardiac evaluation was carried out: EKG was without particularity, and a transthoracqiue echocardiography was normal with a good biventricular function LVEF = 60% and no significant mitro-aortic valve disease.
The patient had received 8 cycles of docetaxel based chemotherapy followed by prostatic radiotherapy with good progress.
Following progressive onset of dyspnea at rest, the patient was referred to cardiology for a cardiac evaluation showing: a balanced blood pressure profile with, on the normal electrocardiogram, (Figure 1) and at transthoracic echocardiography, a severe cardiac hypokinetic with an LVEF of 33% (Figure 2) and altered longitudinal function (Figure 3 A, B) without LV dilation, and moderate aortic and mitral insufficiency (Figure 4).
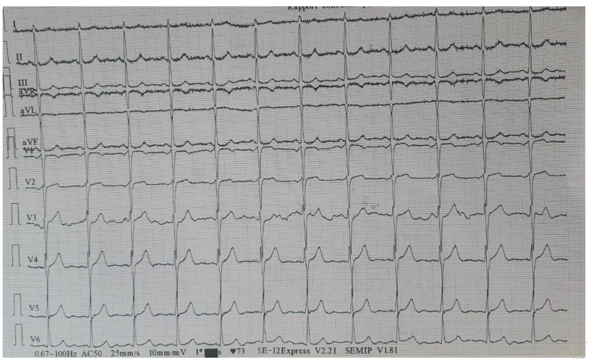
Figure 1: Normal electrocardiogram
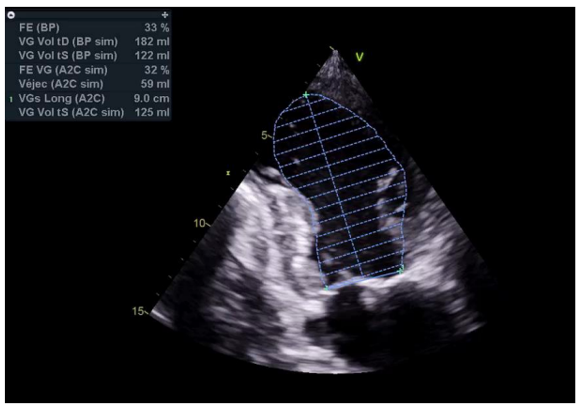
Figure 2: Severe cardiac hypokinetic with LVEF = 33%
A cessation of chemotherapy was indicated, and we started a treatment of heart failure based on bisoprolol 2.5mg 1 tablet/day, ramipril 2.5mg 1 tablet/day, anti aldosterone 50mg 1/2 tablet/day with a reassessment of the LVEF after 2 months which showed a marked improvement in dyspnea, with an echocardiography of LVEF at 40%.
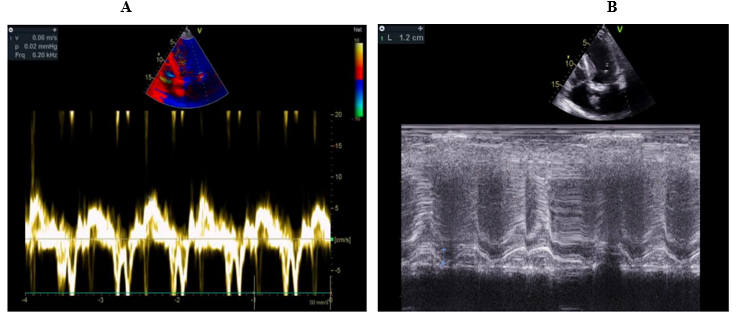
Figure 3: Altered longitudinal function (A) S’VG = 6cm/s (B) MAPSE = 12mm.
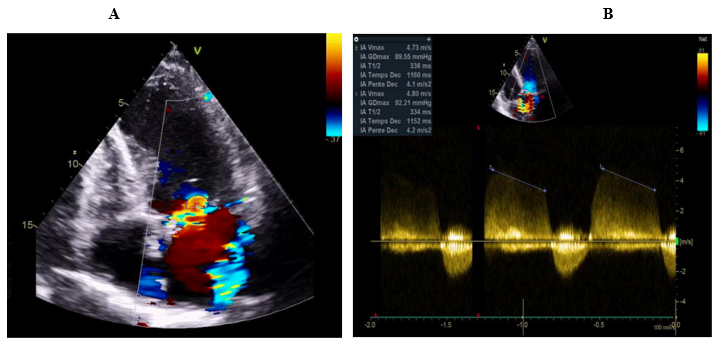
Figure 4: Moderate mitral (A) and aortic (B) insufficiency
The biological assessment was normal, with Hemoglobin: 12.5g/dl, c-reactive protein: 5mg/l, ultrasensitive troponins: 3 ng/l.

Figure 5: Normal Coronary angiography
Coronary angiography was performed returning normal (figure 5).
Docetaxel cardiotoxicity is retained in this context.
Discussion
Cancer remains a public health problem today. Considerable progress in cancer treatment has increased the life expectancy of patients at the cost of short- and long-term cardiovascular adverse effects [2].
Among the most widespread cancers in the world, prostate cancer, which continues to increase with the increase in life expectancy and the evolution of therapeutic strategies.
Nowadays, the systemic treatment for prostate neoplasm consists of hormonal therapy, chemotherapy, immunotherapy, radiopharmaceuticals and targeted therapy. several of these treatments carry a risk of cardiovascular complications that limit their use [3].
Taxanes are part of the therapeutic panel used to treat prostate cancer. Docetaxel and paclitaxel induce cardiotoxicity in 2.3% to 8% of patients. They are mainly used in the treatment of patients with breast, prostate, lung, ovarian cancer [4].
The mechanism of action of docetaxel resides in the transformation of tubulin into permanent microtubules as well as the inhibition of their degradation. there will be a significant reduction in the amount of free tubulin. This mechanism is responsible for the anticancer activity of docetaxel but can also alter the cardiovascular system. In addition to this direct cardiomyocyte toxicity, docetaxel can induce oxidative stress and endothelial dysfunction via increased cell apoptosis [5].
A study of 10 patients receiving docetaxel, or regular monitoring of diastolic and systolic cardiac function and measurement of serum cardiac neurohormone concentrations one day before, one day after, and three weeks after docetaxel administration, confirmed that docetaxel can induce left ventricular diastolic dysfunction and an increase in serum BNP concentration without altering systolic function [1].
Therefore, it is advisable to monitor the cardiac function of patients to be treated with docetaxel by echocardiography. In addition, serum BNP may be a useful marker for assessing docetaxel-induced cardiotoxicity [1].
This article is among the first of its kind to elucidate the cardiotoxicity of taxanes and more particularly docetaxel causing heart failure.
Cardiotoxicity induced by taxanes remains rare, unrecognized and often neglected by the practitioner. this clinical case should encourage practitioners to carry out regular cardio-oncological evaluations in patients receiving taxanes in order to detect left ventricular dysfunction which may be asymptomatic.
Conclusion
The field of cardiac adverse effects of chemotherapies has expanded with the development of numerous protocols combining conventional cytotoxics and targeted therapies over the past 20 years.
The emergence of the subspecialty of cardio-oncology is the result of the awareness that patients treated for cancer represent a high cardiovascular risk and aims to prevent, detect, treat and monitor cardiovascular complications secondary to chemotherapy.
References
- Shimoyama M, Murata Y, Sumi KI, Hamazoe R, Komuro I. Docetaxel Induced Cardiotoxicity. Division Of Cardiology, Department of Medicine I, Tottori University, Faculty of Medicine, 36-1 Nishi-Machi, Yonago. 86(2). [Ref.]
- Siegel R, Desantis C, Virgo K, Stein K, Mariotto A, et al. (2012) Cancer Treatment and Survivorship Statistics, 2012. Ca Cancer J Clin. 62: 220-241. [PubMed.]
- Alibhai SMH, Duong-Hua M, Sutradhar R, Fleshner NE, Warde P, et al. (2009). Impact Of Androgen Deprivation Therapy on Cardiovascular Disease and Diabetes. J. Clin. Oncol. 27: 3452-3458. [PubMed.]
- Todaro Mc, Oreto L, Qamar R, Paterick Te, Carerj S, et al. (2013) Cardioncology: State of The Heart. Int J Cardiol. 168: 680-687. [PubMed.]
- Parker C, Nilsson S, Heinrich D. (2013) Alpha Emitter Radium-223 And Survival in Metastatic Prostate Cancer. N Engl J Med. 369: 213-223. [Ref.]